urologist seen at clinic
I’d try starting with 100mg per week. Split it into two doses every 3.5 days if you want. Wait at least 8 weeks, and evaluate from there.
1 Like
1000
Good conclusion.
But she was half right in terms of weekly equivalent dose. Take the 300 /4 which gives you 75 mg per week of test ester.
Given we know nothing about you the responsible estimate for suggested starting dosage per week would be 75-100 mg/week of test ester. No, not a starting dose of 150 mg/week and no not a starting dose of 200 mg/week.
Nice job @cliteastwood!
For more info, see here and below:
Get your bloodwork done in the timing @cliteastwood shared and if you really want to be diligent check your peak and trough and dial in your protocol based on (1) symptom relief along with (2) prior knowledge of your (if applicable) eugonadal TT/fT range, and (3) constraining your TT/fT levels based on your risk tolerance understanding that the higher you go outside the male reference range the more risk you may be taking on in terms of long-term cardiovascular health.
1 Like
1000
1 Like
If she is receptive and you feel knowledgeable enough I would tell her how you would like to be treated. That is what I did, My doctor wanted me on cream and I asked for shots and told him the frequency I wanted and they listened.
What about Jatenzo?
1000
1 Like
I wish you the best. More reading on various administration options and their estimate PK profiles vs a hypothetical young and old males:

I don’t know what that is. It wasn’t offered. I’m good with the protocol we settled at. They pretty much let me run the show and keep an eye on my bloods to make sure all is going good. I pay cash for their service. Feels good to have a doctor work for me instead of my insurance. I actually get good treatment. Wish I could say the same about my GP.
1000
Good luck. Keep this updated!
1 Like
Anything you need let me know.
1000
1 Like
Actually you are a pretty typical eliminator of free T if the data point you provided is TT in ng/dl after 10 days. Also you have to consider that if the upper reference range for the assay is ~800 ng/dl it may not have parity with gold standard LC/MS-MS assay (LC/MS-MS assay may read higher or lower than your assay). It’s all very arcane.
Nevertheless I’d place you below 50% of age adjusted study study group given your data point meaning you are a reasonably good eliminator of fT. Testosterone will build up over time in every patient based on the elimination half life of the ester (in this case I’m assuming about 4.5-5 days for Testosterone Cypionate/Enanthate).


1000
1 Like
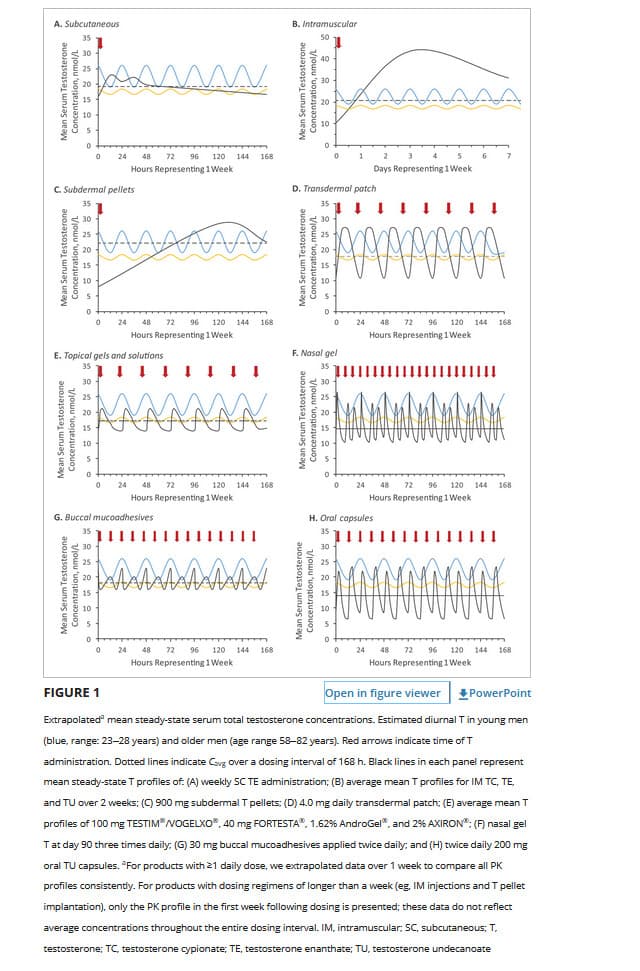
As shown, if you want to best mimic young male physiology (circadian rhythm) you’ll need to go with an application route that has short apparent elimination half life (1-6 hours) that comes with using pure testosterone instead of the ester. Either oral troche (buccal) admin, cream, nasal gel, test suspension, capsule all come with their pros and cons and once daily admininstration in the AM will insure your levels are back to baseline by night. Nasal gel has also shown promise in restoring HPTA function in some men that may also have subjective benefit.
You don’t have that flexibility with the injectable ester but if you inject everyday you will have near constant blood levels of T 24 hours a day. For some men this is problematic for sleep.
1 Like
1000
1 Like
1000
I think going from the shot frequency you were at to once or twice a week will be a world of difference.