What is the range for their e2 test?
Great. @increasemyt post your email in the about me section and I will have someone contact you, if not myself.
@increasemyt - I just got my most recent bloods back. I’m taking 40mg EOD, 4mg tadalafil and 90mg armor thyroid for hypothyroidism.
Generally speaking, I feel great… But there have been times recently mid sex that I’ll lose my erection. Also, there are times it takes me forever to orgasm and when I do, the volume is very low. Also, I’ve had a vasectomy.
Thoughts on my noodle going limp mid sex and the other things?
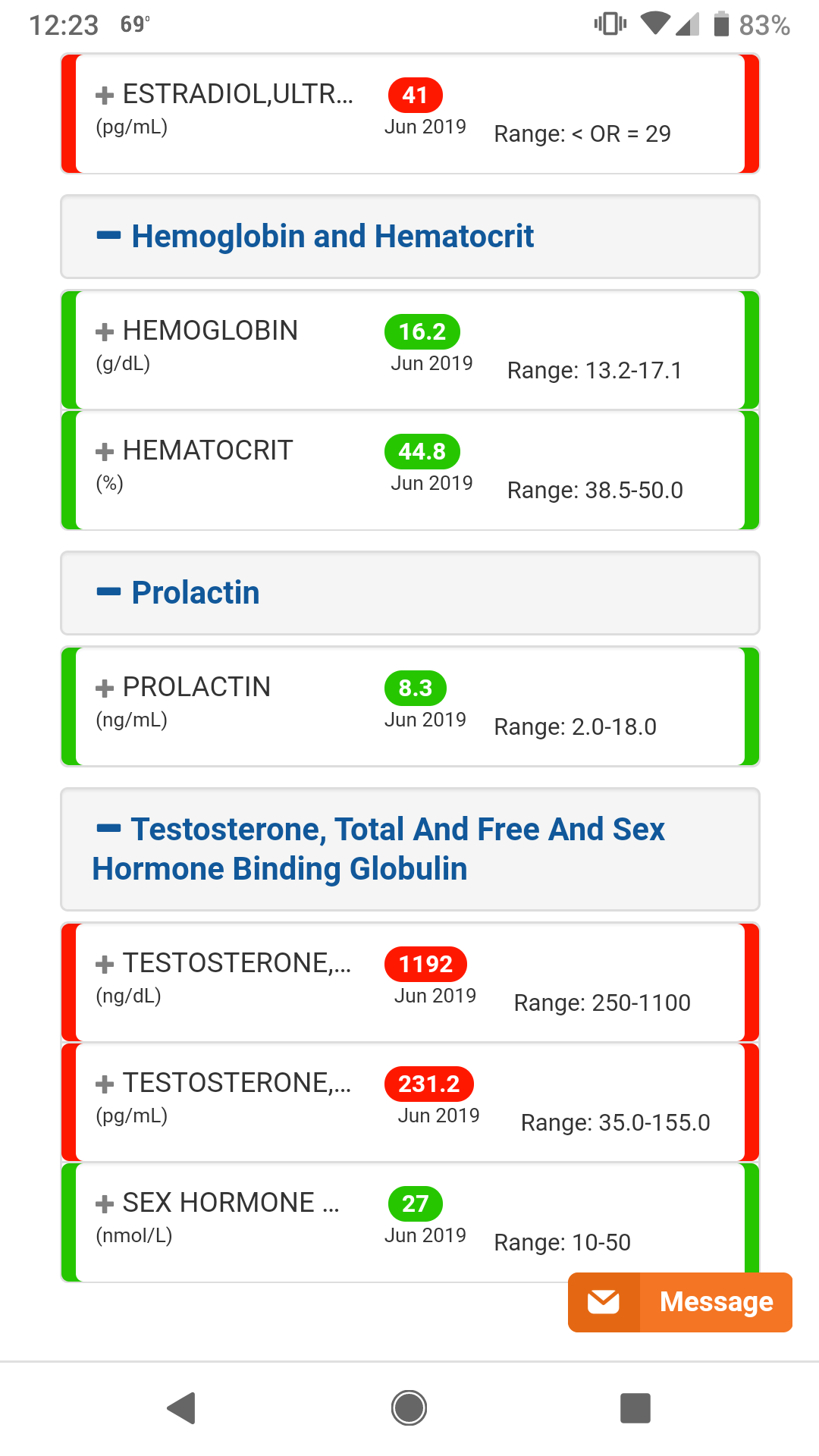
It is the standard sensitive assay range. They would obviously be considered way over range. We don’t use ranges. We increase dose until symptom resolution. Your ideal dose will differ from everyone else. Typically, men have symptom resolution once free T gets to 30 ng/dL. The guys doing the best are at 40 ng/dL.
So is the range used the one <29 for e2?
If so I would agree those numbers are way way over range.
Tell me you’re history. How long you have been on, what your protocol is, what changes were made.
Also what is your history before TRT.
This info will help, but my initial guess is that your estradiol is too high because that is a sensitive test 28 is the sweet spot.
Also, you could probably lower your dosage some.
one thing @dbossa is finally right about, is E2 is different for everyone symptomatically. Some people can have really high E2 and have no symptoms, that does not mean it is ok to let your E2 run rampant as it is implicated in male breast cancer and prostate cancer.
You’re free T is at 23 ng/dL. My symptoms resolved once they got to 28 ng/dL. You may just need a higher dose. I also got better symptom resolution moving to ED from EOD.
Higher dosage? What are you talking about his free T is 150% + the range.
Expert commentary
Our understanding of estrogen’s function in the pathogenesis, prevention and treatment of prostate cancer is still evolving. Although androgens are clearly involved in the progression of prostate cancer and anti-androgen therapy will probably remain the treatment of choice for metastastic disease for the foreseeable future, it is equally clear that androgens are only one side of the story. At least in rats, testosterone alone is necessary, but not sufficient, for the development of prostate cancer. It is only with the addition of estrogen that cancer can be reliably induced. In vivo and in vitro studies have identified multiple mechanisms of potential carcinogenesis, including direct genotoxicity, epigenotoxicity, hyperproloctinemia, chronic inflammation and prostatic ER-mediated changes that are in addition subject to disruption by environmental estrogens. Moreover, ample evidence for estrogen’s role in the development of human prostate cancer exists in the form of epidemiological data and associations between inflammation and cancer, which parallels findings in rodent prostates. The true role of estrogen in prostate cancer development and progression is probably complex and multifactorial, incorporating more than one of the mechanisms already described and with interplay between them.
So all men who don’t take an aromatase inhibitor are at increased risk for prostate cancer? We should all be taking an AI to lower that risk?
Again, are you serious? You can’t possibly be serious.
No I never said that, and your post highlights your confusion on the subject.
A high level of one type of estrogen in a man’s body might increase his risk of developing prostate cancer. That is one surprising conclusion from a new study which also offers another novel finding – that high levels of the estrogen considered fuel for breast cancer might offer a protective benefit against prostate cancer.
**Kosti says her team also observed that the estrogen metabolites considered as ‘harmful’ estrogens in breast cancer (**16-KE2 and 17-epiE3) are secreted in higher amounts among those without prostate cancer and in lower amounts in those with prostate cancer.
Does a man’s estrogen level impact his risk of prostate cancer?
I can assure you that I am not confused. I understand this process quite well.
I will use the email from the site. The one that starts with info. Fair enough?
I know exactly who you would do this podcast with. Once you’ve been properly schooled, I’ll be curious to see if you return here and confirm you were dead wrong. Looking forward to seeing that.
Yup. I cant find the about me section right now.

Been on TRT for almost 2 years. Went to urologist for ED and total T tested 250ish 3 separate times, so he prescribed test cyp. Started at 100mg a week and have moved up to 140mg a week.
I inject 40mg EOD sub-q, no HCG, no AI.
History before TRT - exercised on and off for about 10 years. Early on, was in good shape but got lazy once I was married/had kids. My diet and drinking also had an ebb and flow during this time going from good eating/no drinking to crappy eating/frequent social drinking.
Currently, I’m 176 and about 19-21% BF according to my scale. I have room to improve my diet and fitness for sure, which I imagine can only help.
I will say, my erections are generally great and I’m ready to go much better than I was before. Had a bump in the road last year, but been taking 40mg EOD since January and I feel great other that the limp dick mid sex episodes.
Interesting to know, thank you.
This stuff is so confusing sometimes. I appreciate you taking the time to respond @increasemyt.
Maybe I’ll have to lower the dose a tad and work on natural ways to clear excess estrogen.
Thanks again
One thing that is strange is your TT and free T is really high but your HCT is not very high. Did you suffer from anemia before TRT?

@increasemyt - did they ever isolate/identify which type of estrogen caused this? (E1, E2, E3)
“This suggests that these particular estrogens may have a protective role against prostate cancer development,” explains Kosti. “It is possible that different tissues respond to estrogens different ways, therefore the potential role of 16-KE2 and 17-epiE3 in prostate cancer prevention and management should be further explored.”
I think they break it down into 15 different types of estrogen. But some variations of E2 were implicated, also E3
The truth is we do not need a study to understand this is what happens. If it were testosterone that gave men prostate cancer then every 21 year old on the planet would be getting prostate cancer, but thats not when prostate cancer occurs.
It occurs when TT to E2 ratios are diminished. So it is obvious estradiol is responsible, it also explains the confusion on why they thought it was testosterone originally.
There is more literature on the subject that is just the first one I grabbed, I gotta run for a little bit I am out of time but will gather more literature today and post it.
Hope this helps
So they jumped at the idea. I’m in talks with everyone to figure out when everyone is available and then I’ll check with your availability.
You will be on a LIVE podcast with the following people:
Myself
Dr Keith Nichols
Dr Scott Howell
Dr Eric Seranno
Dr Steven Devos
I’ll be in touch soon via email.
Association does not demonstrate causation.
When you say “Because A, then B becomes obvious” is what is referred to as a logical fallacy.