Please provide one study showing what you just said to be true. Let me save you time. You can’t. What in the world do you not get about over 80 years of testosterone studies and the erythrocytosis with it never causing harm in any of them. The fear comes from extrapolating the harm of PCV to erythrocytosis. Show me one study to support your opinion. The actual literature does not support your opinion.
Fire away. You won’t get this anywhere else it appears. Good stuff and happy reading.
What makes you think it’s estrogen ?
You’re talking 7 days versus 9 days for most people not vs 4.5, they are essentially interchangeable (and I have done that when necessary without complication)
You know what caused that for me? Melatonin and those nootropics. Everytine I take them it happens again and again. I stopped taking those. Estrogen does not cause ejaculation issues if actually makes sensitivity and libido better.
2 Likes
I’m not sure what you mean. Can you elaborate?
Can I ask what your free T levels were at the time and what was your exact protocol?
You know I’m really sorry man. If you didn’t word your posts as such where you are so fucking condescending, I might could actually read between the lines and actually listen to whatever your point is supposed to be.
I love that you have you passion Danny. I love that you have researched the hell out of things. I sincerely applaud that. If you weren’t such a DICK we could all probably learn something from you.
My comment regarding this was a reason, not an excuse. You talk about keeping things simple. I don’t want a fucking FB account. Simple…
If you guys can’t provide another option for correspondence (which is fine one way or the other) , then I guess I just won’t be one of the elite! Lol. Don’t tell me I “have no excuse” like I’m some kind of fucking kid that skipped out on mowing the lawn. Geez and you wonder why people can’t accept anything from you?!
4 Likes
Might not be estrogen at all. Let me rephrase - do you have any thoughts about deceased ejaculate and taking forever to finish in relation to higher levels of testosterone?
When I increase my dose, ejaculate volume decreases and time to finish more often than not increases.
Only variable I change is dose size. Could it be something different down stream as a result of more testosterone? Something that effects the prostates ability to generate ejaculate?
Thanks
All of those issues vanished once I moved to daily injections and significantly increased my dose. That’s why I asked the question of your free t levels and exact protocol.
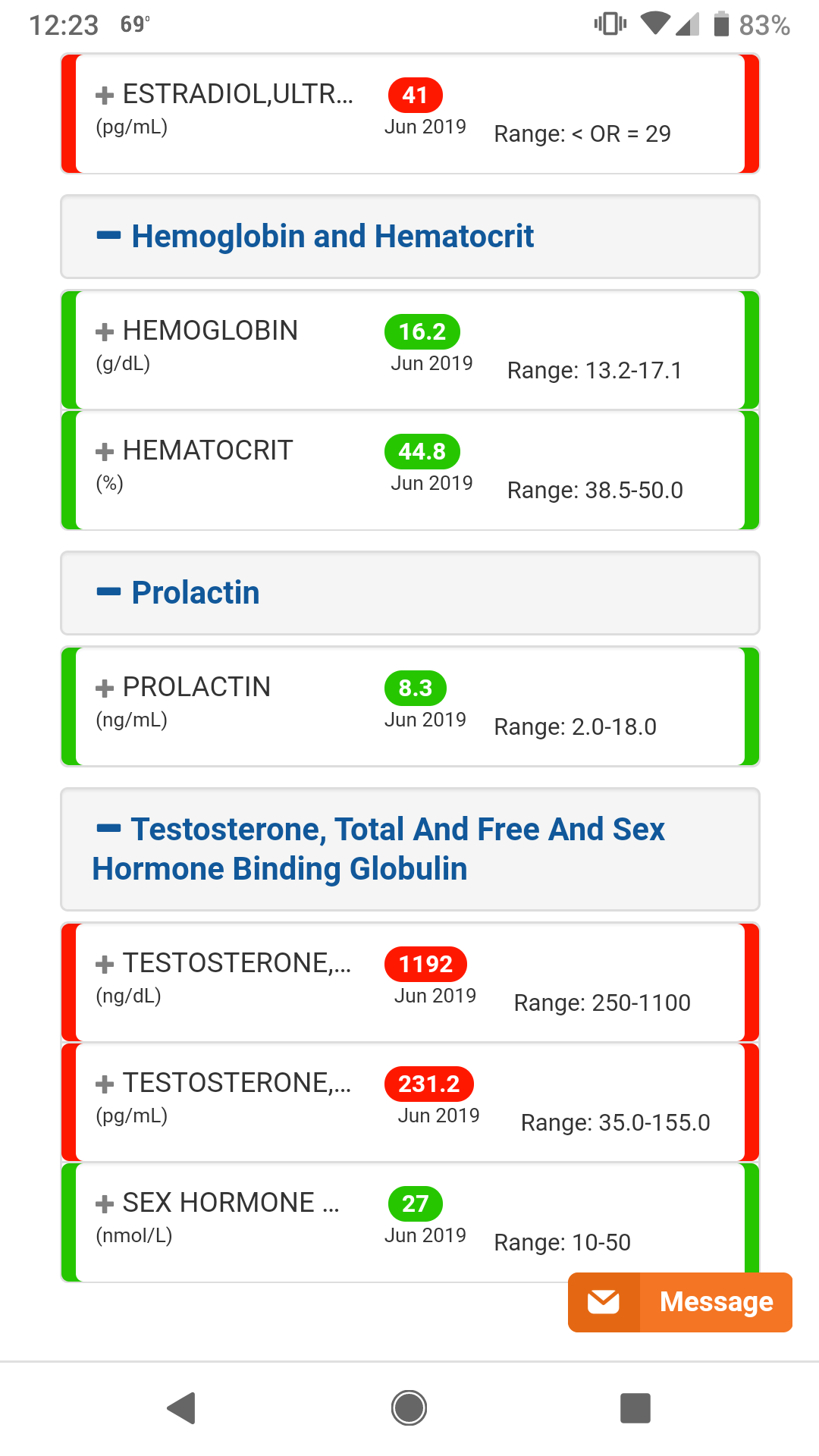
Most recent bloods. Supposed to be 40mg EOD and nothing else, but I may have overfilled syringe a few times to 42 or 44mg during backfill and just injected the dose.
1 Like
Fixed the issue with the graphs as I had to recopy them.
Was that absolutely necessary? Are you that miserable on your current protocol that you felt compelled to react that way to my post?
When you signed up here, did you not have to open an account, answer a bunch of questions, create a fake name, etc? What would be so different creating a similar one there to have direct access to some of the top doctors in the world? There are plenty of guys there that have a fake Facebook account simply to have access to the wealth of information there as they wouldn’t use the account for anything else. All the info is there, the docs are there, over a thousand pre-screened members, research papers, etc. So, if ever someone wanted to access to such things, for free, there is really no excuse. If you don’t want to have an account there nobody is putting gun to your head. I was just putting it out there for anyone interested. I wouldn’t have suspected for one moment such a crass comment like that. I help people every day. I usually get thanked. Not insulted. You are more than welcome to skip over any of my comments here. You are under no obligation to do anything you don’t want to do.
Your free T works out to 23.1 ng/dL. I only began to experience symptom resolution once I hit 28. Miles better doing daily versus EOD. My free T is currently over 40 and all symptoms resolved across the board. In your case, I would do 25mg daily and give it 6 weeks to assess.
I was just saying thanks for taking a look and sending it over. Hope it helps explain relevant variables at play in determination of blood viscosity:
Hct + inflammation (increase plasma viscosity) —>elevated blood viscosity —> potential issues depending on the patient.
You can’t make a blanket statement that erythrocytosis is harmless. I mean you could but you’d be wrong. And if you are wrong with certain compromised patients, you would be doing harm. Not good to make blanket statements.
Feel free to correct any errors.
No it wasn’t. Neither is it necessary for you to condescend others on here brother. Everyone here deserves, at the very least, the respect of common civility. You have crossed that line many times here. That’s my ONLY problem with you.
Regarding FB…AGAIN, I’m a grown man. If wanted a FB account, I’d have one. I don’t want it. I don’t have it. I ain’t gonna. It’s just that simple brother. I don’t owe you or anyone else an explanation of why that is, it just is for me because I said it is…for me.
And no, I didn’t use a fake name to join here. Not at all. Again, I’m a grown ass man, not a child hiding in the corner. I have nothing to hide or any reason whatsoever to maintain anonymity. Some people do. More power to them. That’s not me. If there’s something about me that I don’t want you or anyone else to know, then you won’t know it. Who I am and what I believe…that’s just me and I really don’t give two shits what anyone else thinks about that you know?
2 Likes
Throwing this out there in case you have never seen it before:

All of my posts are directly in response to it. Thanks for reposting it.
Oh I forgot to mention…my current protocol is fine and I feel great. And thank you for putting more thought into your last post. See? It’s not that hard to be nice now is it?
Edit…I think I hit reply to the wrong post…
This was meant for @dbossa
Lots of posts going back and forth here.
Hct + inflammation (increase plasma viscosity) —>elevated blood viscosity —> potential issues depending on the patient.
Recopied these:
Testosterone use causing erythrocytosis
The implications of the systemic vascular resistance response for the treatment of several anemias have been discussed above. It is also worthwhile mentioning that increased blood viscosity is easily treated with therapeutic phlebotomy [Holsworth et al. 2014]. This intervention has great potential because increased blood viscosity is seen in association with all major risk factors for atherosclerotic cardiovascular disease [Sloop et al. 2015]. Therapeutic phlebotomy is not an obsolete modality from medieval times. Sir William Osler used it in treating pneumonia at Johns Hopkins Hospital. This quote is from the 1921 edition of his classic textbook, The Principles and Practice of Medicine :
We employ [therapeutic phlebotomy] much more than we did a few years ago, but more often late in the disease than early. To bleed at the very onset in robust, healthy individuals in whom the disease sets in with great intensity and high fever is good practice. Late in the course marked dilatation of the right heart is the common indication [Osler and McCrae, 1921, p. 102].
The benefit observed by this eminent clinician was probably due to a decrease in elevated blood viscosity caused by the acute phase reactant fibrinogen, which would improve vascular congestion as well as decrease pulmonary vascular resistance in cor pulmonale. Therapeutic phlebotomy was used for angina pectoris at Charity Hospital in New Orleans in the 1960s [Burch and Depasquale, 1965]. Those patients reported a general feeling of improvement in wellbeing after phlebotomy. Additional reports of the efficacy of therapeutic phlebotomy in angina pectoris were published in 1970 [Parker et al. 1970] and 1994 [Piccirillo et al. 1994]. Most recently, a prospective, randomized trial of therapeutic phlebotomy in metabolic syndrome resulted in significant decreases in serum glucose and blood pressure [Houschyar et al. 2012]. Systolic blood pressure decreased from 148 ± 12.3 mmHg to 130 ± 11.9 mmHg in subjects and from 144.7 ± 14.4 mmHg to 143.8 ± 11.9 in controls. Serum glucose decreased from 110.7 ± 29.4 to 98.5 ± 24.0 mg/dl in subjects and from 109.1 ± 39.4 to 107.3 ± 33.6 mg/dl in controls. Furthermore, blood donation is also associated with a reduced risk of myocardial infarction [Salonen et al. 1998]. Although prospective data on therapeutic phlebotomy, blood donation and blood viscosity on the risk of atherosclerotic cardiovascular disease are still either limited or not widely appreciated, hemodynamics must obey the laws of physics: perfusion is inversely proportional to blood viscosity, and without a response to maintain homeostasis, blood viscosity will increase systemic vascular resistance. Reduced blood viscosity will increase blood flow to skeletal muscle, increase glucose utilization, and improve hyperglycemia. Therapeutic phlebotomy will decrease systemic vascular resistance and blood pressure, whatever the cause.
The role of chronic hyperviscosity in vascular disease
Conclusion
Cardiovascular disease is still the leading cause of deaths for both men and women worldwide. Many risk factors have been identified and current therapeutic efforts have been centered on addressing these risk factors. However, as of today, the role that blood viscosity plays in this disease has not yet received its due attention. Viscosity is a fundamental property of any fluid. Its important role in both normal individuals and patients afflicted with cardiovascular disease has been underestimated. Past and current research has reported the benefits in addressing this important factor; however, mainstream medicine has not appreciated or fully accepted this important measurement. With continued research and published, peer-reviewed studies pertaining to the importance of blood viscosity in cardiovascular diseases, this relationship will be recognized, appreciated and will no doubt reveal the positive aspects of hemorheology, which will save lives.