@anon18050987 there is still a statement of yours from way up above that I will address (ranges). I believe @yeti308 has probably clarified several things.
There is no better individual on this entire forum to teach you this stuff. None. I’ll bet my life on it.
Heading back to my office now and I’ll reply there.
Let me just address the important one. The erythrocytosis from testosterone is not dangerous (it’s beneficial) and has never caused a problem in the
History of testosterones use. The physiologic erythrocytosis has never caused a problem. That’s my point.
Once again a great theory and concept but hasn’t played out in any study when we raise he hb and hct in any study including men with cardiac disease. So much more involved such as the pliability of the rbcs etc. So with regard to TRT the erythrocytosis has never caused harm
@anon18050987 you need to differentiate erythrocytosis (harmless) which is normal and to be expected, to a certain degree, with TRT use vs polycythemia vera (harmful) which involved a clotting issue. Men with erythrocytosis have no need to donate. Guys at altitude wind up with higher levels. Elite athletes using depo etc wind up with higher levels. None of them are dropping dead. Guys at altitude are not lining up at the blood bank. We monitor levels if they start getting high to simply ensure it is erythrocytosis and not something else.
@yeti308 - do you have any thoughts about deceased ejaculate and taking forever to finish in relation to higher levels of E2?
I’ve had a vasectomy too…seems when I’ve increased my dose (assuming an increase of E2 as well since there is more test to convert) I always have a decrease in volume and there are times I have a hard time finishing.
I think this has also happen to @alldayeveryday and @NH_Watts too. Curious if there is some link to E2 and decreased volume/increased duration to finishing?
Hcg doesn’t work for many and adding HCG to a protocol complicates things. If a man is having that much pain I’m sure Dr. Yeti would give the man HCG. Actually I know he would.
Simplicity is the key. Not the nonsense that goes on with “inject Monday and thursday and then add HCG on Tuesday and friday. At the same time apply part of this cream to the inside leg, just in case you have estrogen issues take an ai. .
Guys, and @anon18050987, as you may have heard, I do some very simple English podcasts on the subject these days. I’m going to post the links to two of them I’ve done which are on YouTube (doubt the mods here will mind). Watch these, then send me your questions. This will prevent me from having to repeat a lot of it. Yes, I made some mistakes of saying ‘estrogen’ instead of ‘testosterone’ (and vice versa), as public speaking is harder than you’d think if you’ve never done it. I await your questions.
Please provide one study showing what you just said to be true. Let me save you time. You can’t. What in the world do you not get about over 80 years of testosterone studies and the erythrocytosis with it never causing harm in any of them. The fear comes from extrapolating the harm of PCV to erythrocytosis. Show me one study to support your opinion. The actual literature does not support your opinion.
You’re talking 7 days versus 9 days for most people not vs 4.5, they are essentially interchangeable (and I have done that when necessary without complication)
You know what caused that for me? Melatonin and those nootropics. Everytine I take them it happens again and again. I stopped taking those. Estrogen does not cause ejaculation issues if actually makes sensitivity and libido better.
You know I’m really sorry man. If you didn’t word your posts as such where you are so fucking condescending, I might could actually read between the lines and actually listen to whatever your point is supposed to be.
I love that you have you passion Danny. I love that you have researched the hell out of things. I sincerely applaud that. If you weren’t such a DICK we could all probably learn something from you.
My comment regarding this was a reason, not an excuse. You talk about keeping things simple. I don’t want a fucking FB account. Simple…
If you guys can’t provide another option for correspondence (which is fine one way or the other) , then I guess I just won’t be one of the elite! Lol. Don’t tell me I “have no excuse” like I’m some kind of fucking kid that skipped out on mowing the lawn. Geez and you wonder why people can’t accept anything from you?!
Might not be estrogen at all. Let me rephrase - do you have any thoughts about deceased ejaculate and taking forever to finish in relation to higher levels of testosterone?
When I increase my dose, ejaculate volume decreases and time to finish more often than not increases.
Only variable I change is dose size. Could it be something different down stream as a result of more testosterone? Something that effects the prostates ability to generate ejaculate?
All of those issues vanished once I moved to daily injections and significantly increased my dose. That’s why I asked the question of your free t levels and exact protocol.
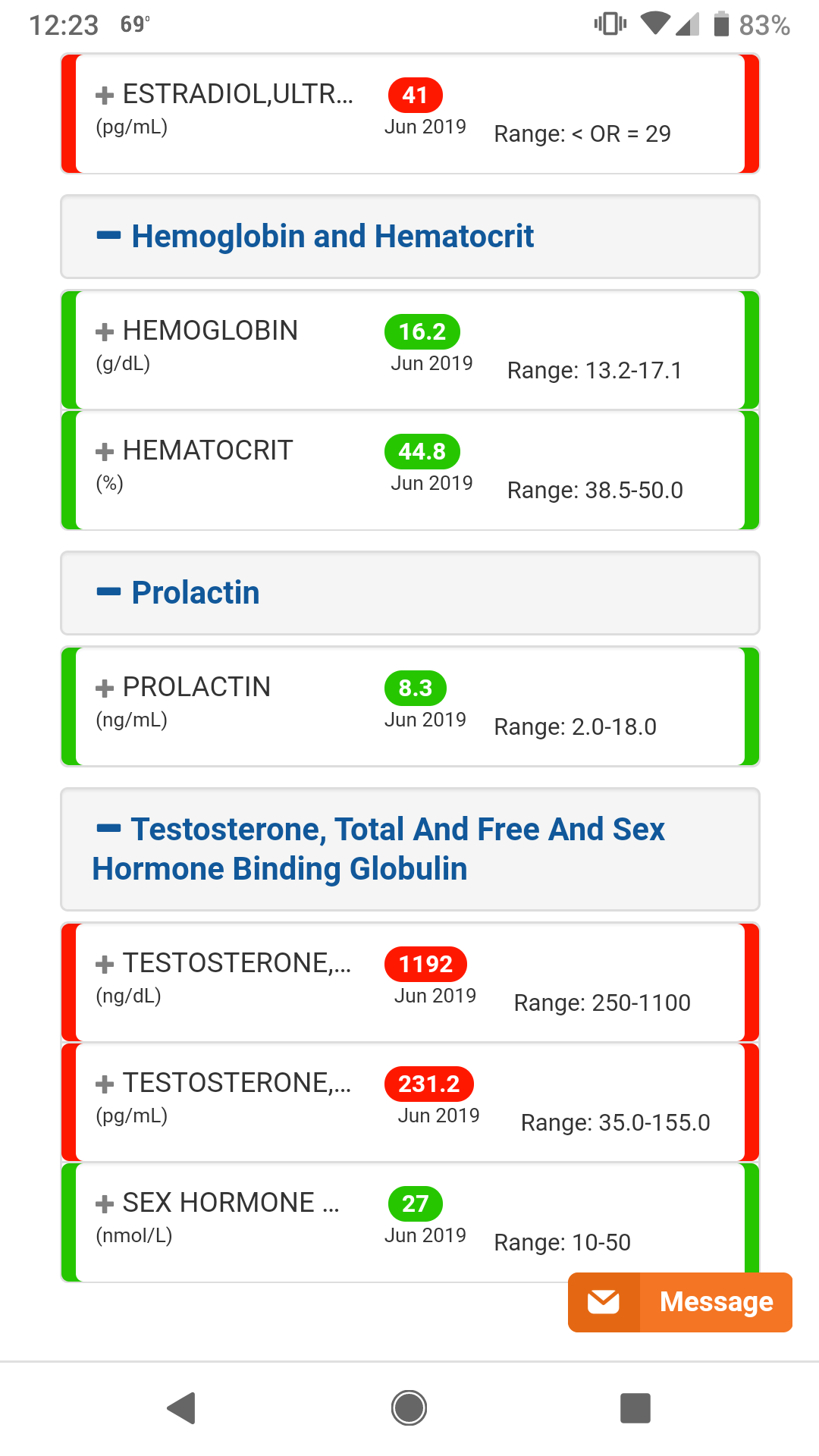
Most recent bloods. Supposed to be 40mg EOD and nothing else, but I may have overfilled syringe a few times to 42 or 44mg during backfill and just injected the dose.
Was that absolutely necessary? Are you that miserable on your current protocol that you felt compelled to react that way to my post?
When you signed up here, did you not have to open an account, answer a bunch of questions, create a fake name, etc? What would be so different creating a similar one there to have direct access to some of the top doctors in the world? There are plenty of guys there that have a fake Facebook account simply to have access to the wealth of information there as they wouldn’t use the account for anything else. All the info is there, the docs are there, over a thousand pre-screened members, research papers, etc. So, if ever someone wanted to access to such things, for free, there is really no excuse. If you don’t want to have an account there nobody is putting gun to your head. I was just putting it out there for anyone interested. I wouldn’t have suspected for one moment such a crass comment like that. I help people every day. I usually get thanked. Not insulted. You are more than welcome to skip over any of my comments here. You are under no obligation to do anything you don’t want to do.