Hello everybody:
I am trying to restart my HPTA after 14 months of TRT (basically, 250 mg of test cyp E2W, no HCG, no AI).
Endo prescribed me 50mg/day of Clomid for 2 months (according to him, this dosage is proportional to my weight, 87 kg 172cm). Then we will do bloodwork. I cannot get Nolva instead, nor HCG.
Taking into account the stickies, I thought 50mg was too high of a dose, so I just took 25mg/day (which is still the double of what the stickies reccommend), because I’m afraid of leydig cell desensitization from high LH.
During TRT, my balls suffered medium shrinkage. However, they were always rather small (9cm3, and 13cm3).
At day 8 of 25mg/day of clomid, I have run bloodwork (01/17/2017):
TT 2,05 ng/ml (2,59-8,16)
LH 2,38 (1,2-8,6)
Estradiol 9 (<53)
My impression is that results might be lower than one should expect. Are those levels normal for the 8th day of Clomid? Should I increase the dose to 50mg/day? How long does it take for Clomid to raise testosterone after being shutdown because of TRT?
Thanks in advance
Your TRT was totally stupid, but we see endos doing crap like this, mindless idiots.
Why are you not self injecting twice a week?
Clomid solo or Clomid+T?
TT suggests solo, but with injections E2W TT could be low if labs were done at end of 2nd week.
On clomid, your hypothalamus and pituitary should react quite fast. LH=2.38 suggests that your hypothalamus and pituitary are not playing the game. In this case, more clomid does not seem harmful other than perhaps some possible increased clomid side effects.
You did not test FT, however E2=9 suggests that FT is really low, reducing FT–>E2
How were you feeling on 25mg Clomid?
You would never use a SERM+hCG at same time.
You might find that your testes work on hCG if you are younger, your details are detached in your other two threads.
Why quitting TRT? I assume because your protocol was wrong, as you would know from the stickies.
The problem is your doctor(s) and you must tackle that issue.
Hi KSman,
Thanks a lot for your help.
Regarding the protocol of 250 mg cyp E2W, that’s the only option they gave me apart from testosterone gel or 250 mg cyp E3W, which I consider even worse. I cannot inject twice a week because test comes in a kind of crystal ampoules which you must break. Then, I don’t know how to save the rest of the dosage in a safe manner for further injections.
Sorry if I didn’t explain well. I am taking Clomid solo (25mg/day), since 01/09/2016, 8 days ago. Last injection of test was 12/21/2016, almost 4 weeks ago. So, I guess all testosterone I have in my system comes now from my own (poor) production.
I suspect I may have some pituitary problem (MRI clear) because of a poor response to a GNRH stimulation test, with 100 micrograms of gonadorelin: LH at baseline was 2.37; at 30 minutes, 7.76 and at 60 minutes, 6.53; FSH was, respectively, 4.93, 7.13 and 7.22. According to doctor, this is a good indicator of pituitary function because there is indeed some response. However, in my opinion, the pituitary response is rather poor.
Yes, I expected LH levels close to 10, not 2.38. So, you think this is a poor response for 8 days clomid, am I right? I’ll try with 50 mg/day and retest in a week.
At 25mg of clomid I feel very low libido, more emotional/depressed and tired all day long. Erections come with difficulties and are medium, not quite hard. Apart from that, maybe because of low testosterone, I am not experiencing other side effects, like visual problems, etc.
I’m 28 years old now, so yes, I could give a try to HCG if I can convince my endo to do so in case clomid/restart fails.
I want to quit TRT because, with this protocol, I get high estradiol, higher blood pressure, my balls shrink, I am/became azoospermic (don’t know if I was before treatment), I even felt sporadically some pressure in my left side of the chest, and specially while sleeping on the side. Without the correct protocol, I’m afraid I will get more harm than health, prostate issues in the long term because of E2, maybe heart problems, etc.
I have tried a few doctors (which finantially is very hard for me) and this is the best I get. I cannot get the drugs by other means.
Thanks again for your time and knowledge.
Best!
There are not multi-dose vials nor vials with the rubber stoppers, but I could try to load multiple insulin syringes. Won’t the syringes get bacteria while being stored? How do I save them, in the refrigerator?
Yes, I did read the sticikes. In fact, I have spent a lot of time and energy reading and trying to find a solution, here, in articles, etc.
I also understand the T+hCG+AI: roughly, T as the main source of testosterone (split low doses for prevent to some degree aromatization and peaks and valleys); HCG low dose to preserve testicular form and function (and some additional endogenous testosterone), and maybe having a better sense of well being; and AI for controlling estradiol, which should be around 22.
Regarding this, the problem is that here in my country, Spain, doctors don’t follow this protocol. From their perspective, estradiol is something irrelevant in males, AI is for cancer, and HCG for fertility (and not in combination with T).
Great video on HCG that i found very interesting. I think he is pretty knowledgeable, but I haven’t had a chance to vet his science. Hope you find it interesting.
250iu hCG SC EOD is ample. Higher amounts may lead to a lot of T–>E2 inside the testes and a competitive AI like Arimidex/anastrozole cannot reduce T–>E2 inside the testes.
Presenter is a hard core BB guy and he injects T with insulin syringes, but I doubt his 100mg T per week!
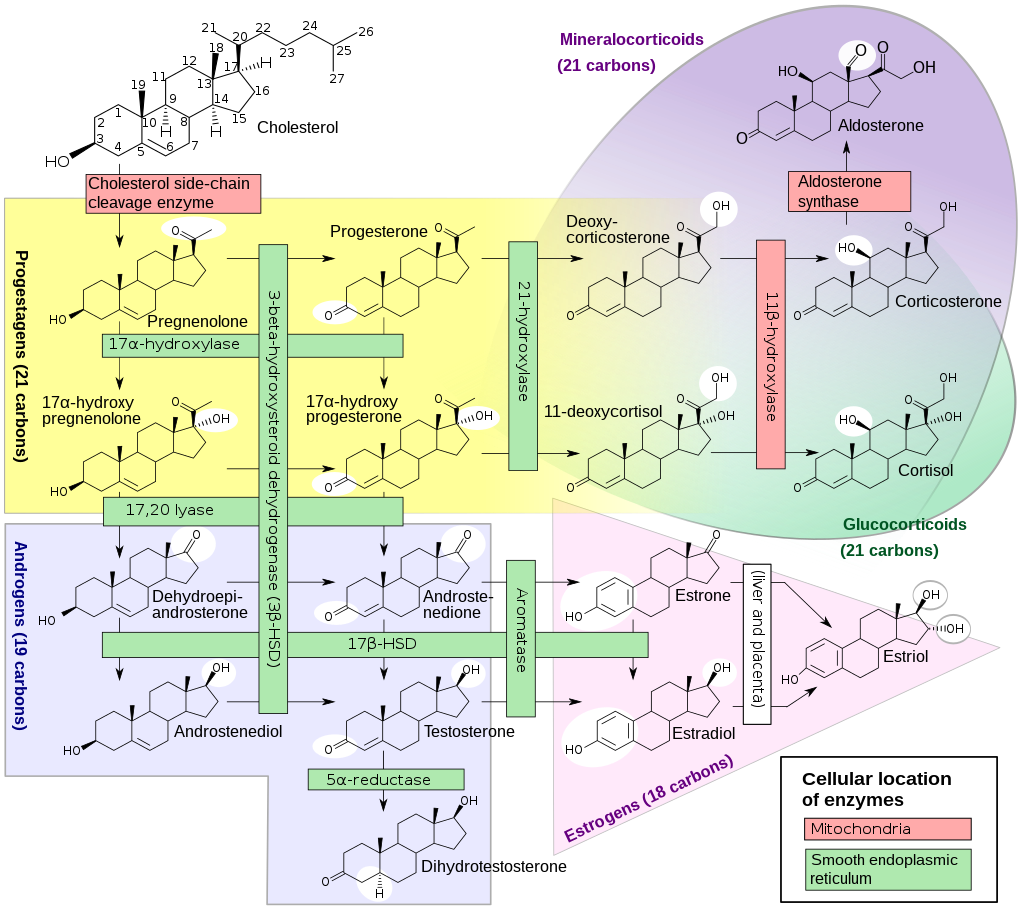
Note that progesterone–>pregnenolone occurs in the mitochondria of all cells in the body, but testicular pregnenolone is significant. Mitochondria also make ATP, the source of cellular energy. Mitochondrial activity is regulated by thyroid hormone fT3 as part of the body’s temperature control loop and CoQ10 made in the liver enables mitochondrial function. So you can see the role of iodine-thyroid.
Update (01/25/2017)
After one week on Clomid 25mg/day and 8 dys Clomid 50/day, TT levels are:
3,99 (2.59-8.16)
I expected a higher number, but there is indeed a increase since last week with TT around 2.
What are your thoughts? Is this a good tendency? Will it continue?
My plan is to keep taking Clomid at this dosage, since it has given good results so far.
Regarding symptons, I still feel low libido and tiredness, but erections, when I perform (which is very sporadically), are sufficient (not as hard as when I was on TRT).
Update (02/13/2017)
I have been on Clomid 50mg/day for 4 weeks (before that, i was on clomid 25mg/day for 8 days). TT levels are:
5,89 (2-59-8.16)
The bloodwork has been done at 14:00, so levels could be still higher in the morning.
Ksman, now I cannot run a complete bloodwork as you suggested, because of money problems. By early March, I hope to do so.
My plan is to stay on 50mg/day since testosterone doesn’t rise much yet, but there is a progression.
Furthermore, I am on a caloric deficit now. Could this lower testosterone levels, despite Clomid? My intention is to reduce body fat and, consequently, aromatization, to try to rise testosterone naturally. I’m not that overweight, but I’ll try this.
Regarding symptoms, I suffer from 0 libido and weak orgasms. I have sex once a week at most, although I live with my girlfriend. On trt, sex was almost daily.
I’ll keep this updated. See you
If LH/FSH are high and T is not, the testes are not performing well. There is a risk of LH receptor desensitization if LH/FSH are too high for a while, a step backwards. Another expected consequence is very high T–>E2 inside the testes with high serum E2 and anastrozole cannot control that.
Your libido is saying that this is not working. Throwing money at labs will not change that.
Update (02/28/2017)
New labs ordered by endo (7 weeks on clomid 50mg/day, excepty by weeks 1 and 6 being on clomid 25mg/day):
TT: 6.7 (2.58-8.16)
LH: 9.37 (1.2-8.6)
FSH: 7.2 (1.3-19.3)
Prolactin: 6.68 (2.6-13.3)
TSH: 1.66 (0.34-5.6)
T4 free: 0.81 (0.54-1.24)
The next step is to stop clomid (from today), and retest in mid April to see where my baseline levels sit.
What can I expect taking into account these results? Any thoughts on them? Should the clomid effect be cleared from my system in 6 weeks?
I’ll keep this updated. Thanks in advance
yes please keep us posted…
I too am attempting a restart after a bumpy ride… 7 years of sporadic t cyp injections roughly 200 mg every week to two or whenever I felt low libido… was never COMPLETELY shut down as I’ve birthed two children in the last 10 years! Most recent cruise was t pellets plus t cyp and t prop as needed… WHAT A MESS… unstable t levels in the 2-4000’s… misuse of ai’s (arimidex/Aromasin) whatever was available… E2 levels all over the place…and to top it off a one month course of tren A and mast P just to experience the libido!!! WHEN… THE EXACT OPPOSITE happened! Dead dick… progesterone up above normal, prolactin up to upper limit of normal…,
Balls small and believe it or not, penis took a hit too! Loss of girth and length… I’m 46 and look like I have 11 year old genitalia!!! I believe the progesterone modulated (up regulated) the E2 receptors in the penile tissue and my genitals took a hit!!! That’s was it for me… enough is enough!!! So two weeks of NO INJECTIONS… I’m starting toremifene asap! Not really pct but a restart protocol, I may make it pct though if I decide to run it for one month or longer…
Doing clomid 25 mg eod as well as its shown to bind and block estrogen on penis, testicles and prostate…
Needless to say depression hit hard but a couple of days in and size is returning quickly to genitals… will be tapering off clomid once size is normal (5-7 days?) and then will continue toremifene for 30-45 days along with Aromasin… I will be very structured with this plan ( for the first time in my life)…no more winging it!
Steroids? NEVER AGAIN! And if this restart doesn’t work, then a really good STRUCTURED Tcyp-hcg-AI
program that I will stick to without playing around!
I’ll run labs at week four! Currently day 2…
I’ll also put up progress notes… libido, ED, function, mood, etc… for those in the same boat!! Don’t mean to steal your post, but we, my friend, are in the same boat!
Current libido poor 1-2/10
Mood? Horrible (from shrunken syndrome!)
Ability to get erect? Probably zippo!
Won’t try until I feel the desire
Hopefully things will take a turn here real soon… based on half-lives… both tren and mast should be ZERO at the end of this week!
Philip3_14, I’m not mean to be rude, but I think you should start your own post if you want to keep a log of your case. Furthermore, in my opinion, we are not exactly in the same boat. I have never used steroids nor played with substances that long, all my testosterone treatment was supervised and guided by doctors. Nevertheless, I hope you to recover too, I’ll keep this updated and I’ll take a look at your log, if you start it.
Best
Update: Labs from 04/05/2017 (1 week ago) :
TT: 2.39 ng/mL (2.59-8.16)
FT:9.6 pg/mL (8.3-40.1)
As you see, TT is low again, so restart didn’t work completely. However, TT seems relatively high for these low TT levels. Does it mean low SHBG?
I’m on hypocaloric diet and lost 11 kg since december. Since FT is not very bad (for sure is not optimal), is it possible that returning to normal diet increases TT and I turn into normal?
Thanks
Update: Labs from 04/12/2017 (almost 1 week ago):
TT: 3.88 (2.8-8)
LH: 2.79 (1.7-8.6)
FSH: 2.9 (1.5-12.4)
Everything else (no more hormones tested by endo) is normal except by:
Neutrophils: 42% (50-70%)
Eosinophils: 7.2 (0-7)
I don’t understad why TT is that higher than 1 week ago from these labs (from 2.39 to 3.88). Any idea? Does it oscillate? I didn’t make any lifestyle change, nor had sex. I still feel hypogonadal. Maybe SHBG has increased.
Antor, I don’t stay on a low dosage Clomid because I’m not sure it is safe long term, and it does not relieve symptoms for me.
Thanks

{kind=link}