Hey Guys,
Looking for some guidance. I’ve been researching on here, but I’m one of those people who don’t trust my own opinion or research on matters like this. I’ve been on TRT for about a year, and showing some effects of high E2 (anxiety, emotion swings, low libido) some time into my TRT (been on it about a year). My labs show Free T on the lower end of healthy range, and E2 on higher end of healthy range (most of the time…see below), so me and my doc were hoping to balance this out more. Here’s the details:
150mg Test Cyp/8 days. Split into a 75mg dose every 4 days, subcutaneous in belly.
Ref Ranges of lab
Total T: 264-916 ng/dL
Free T (Direct): 8.7-25.1 pg/mL
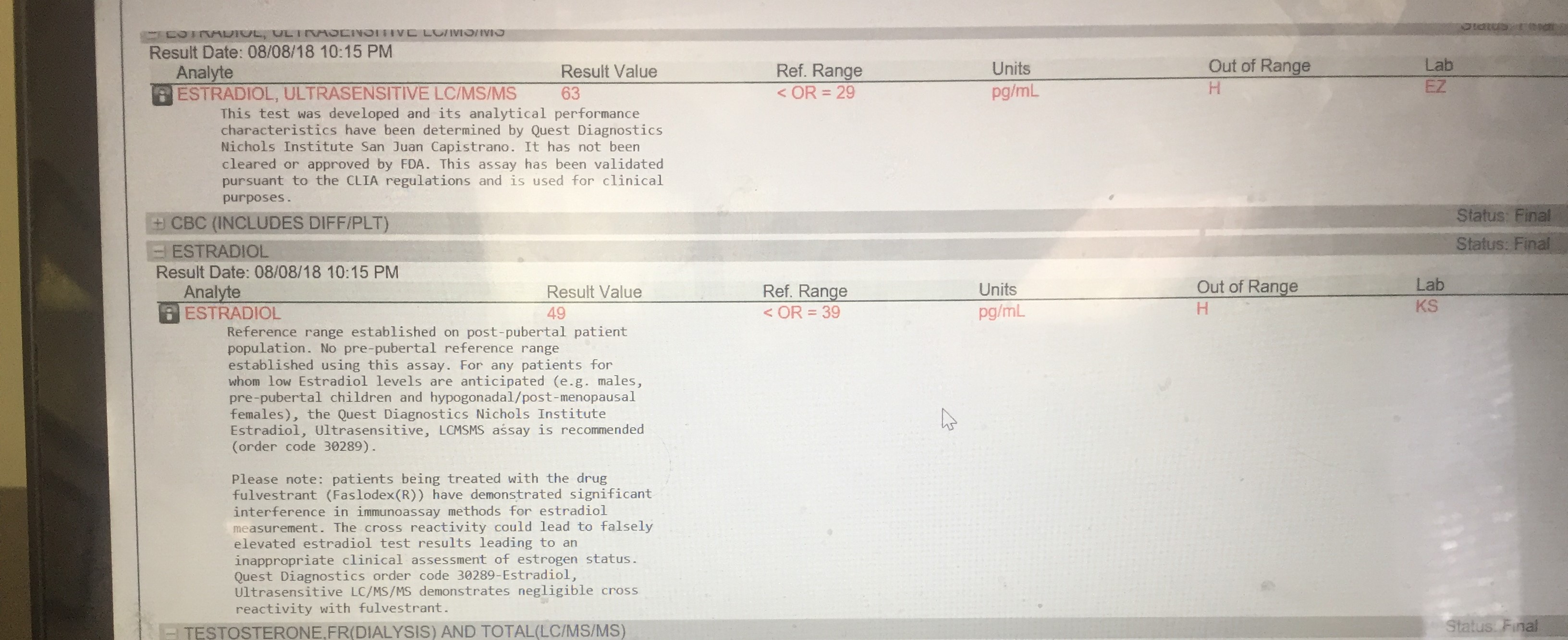
Estradiol : 7.6-42.6 pg/mL
SHBG, Serum: 16.5-55.9 nmol/L
My last two labs results…
-2 days before next injection/2 days after injection:
Total T - 751
Free T - 18.8
Estradiol - 39.8
SHBG - 36.1
-1 day before next injection/3 days after injection:
Total T - 645
Free T - 12
Estradiol - 32.4
SHBG - 34.4
I believe my Estradiol is spiking even higher the day after injection, as I have previous reports that my doctor didn’t mention noticing, like one in April (can’t recall exact timing of bloodwork in relation to injection) with the same dosage and schedule where results are:
Total - 682
Free - 12.8
Estradiol - 43.7 ***
Hoping someone like KSMan or another heavily active user can give some input on how to use the Anastrozole tablets I was just prescribed (1mg). My doc suggested half a pill twice a week. I’ve seen suggestion on here of .25mg twice a week instead, so I’m not sure.
Can some give some guidance on how much and what timing to take this to get the Estradiol lower? Also, will the subsequent effects of lowering Estradiol be higher T levels, or would I still need to inject more to get the T numbers up?
Thanks for the help guys.
EDIT**** - Appreciate the feedback guys. Would there be drawbacks of using the AI? I’ve seen the recommendations of increasing frequency of dosages to help, but if there’s not a major drawback to the AI I’d prefer to go that route, as someone who has issues with needles. Getting it down to 4 days at a time was tough enough due to phobia of sorts, and I still get vasovagal responses a lot of the time even after a year+ of TRT, so I really don’t think I’d have an easy time sticking to every other day… Thoughts?