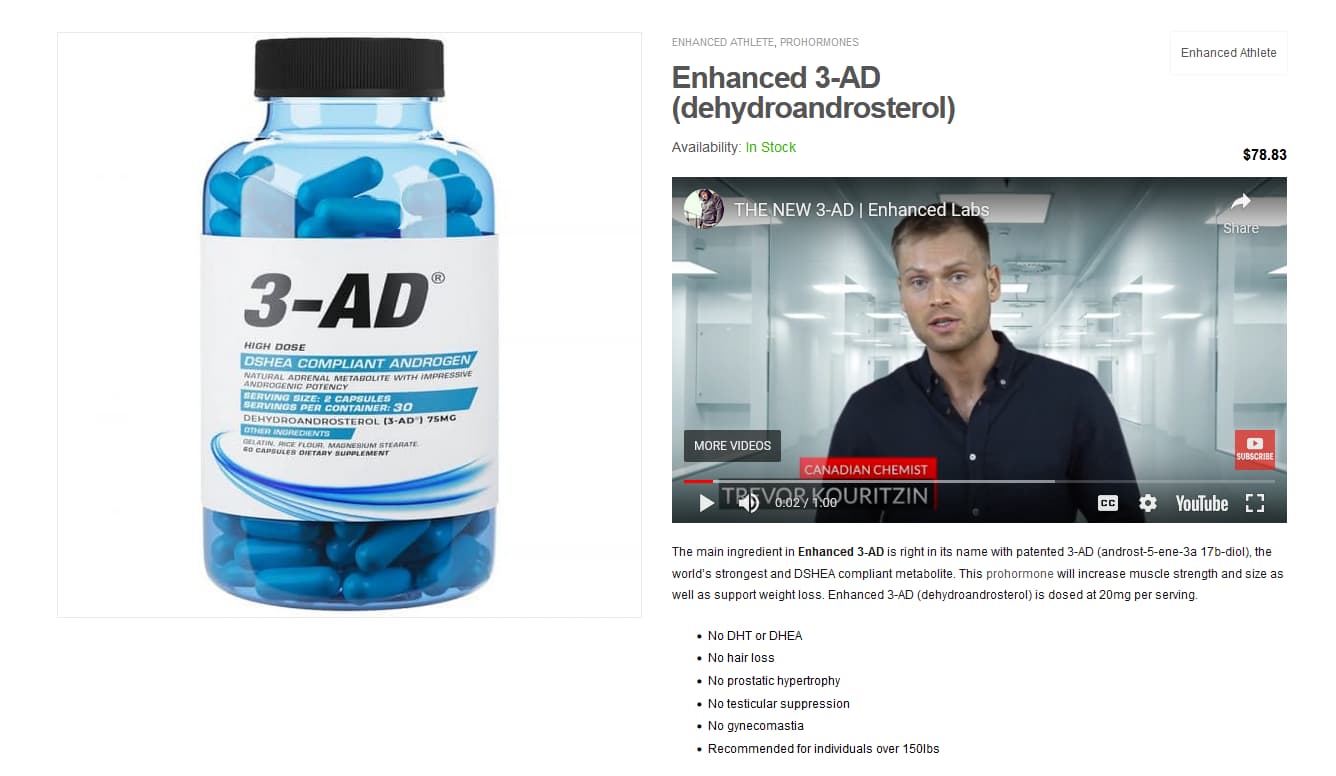
So I purchased 3-AD by enhanced labs. I havent used it yet and wondering if anyone had experience with it or knows any common side effects. A google search didn’t provide me much detail and I’d like to know what I’m getting myself into. Any advice would be greatly appreciated.
Any ‘prohormone’ these days over the counter is snake oil. Sad to say it.
1 Like
Get your money back and tell them you don’t like spending $64-99 for a 60 count bottle of nothing.
Buy 60-100 jugs of RO water instead (very anabolic)!

Wow, sounds impressive:

DSHEA compliant should have tipped you off. They are just playing regulatory games for young people who should take their money and invest in some basic organic chemistry education.
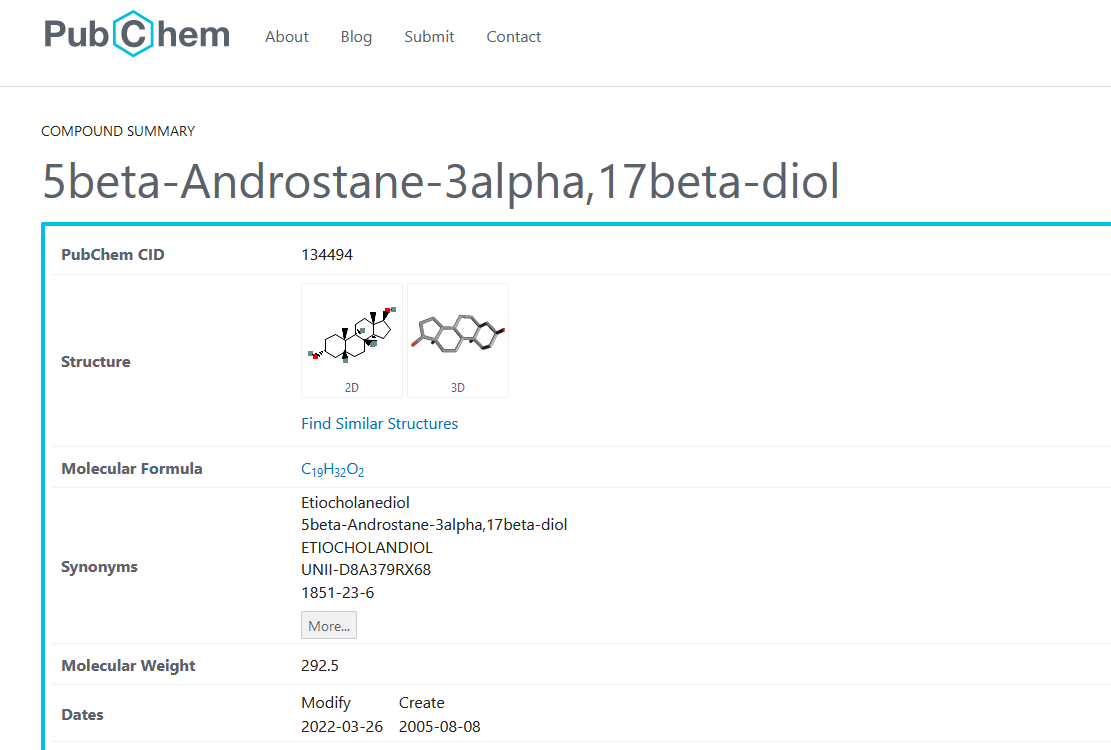
Worthless oral anabolic agent:
2 Likes
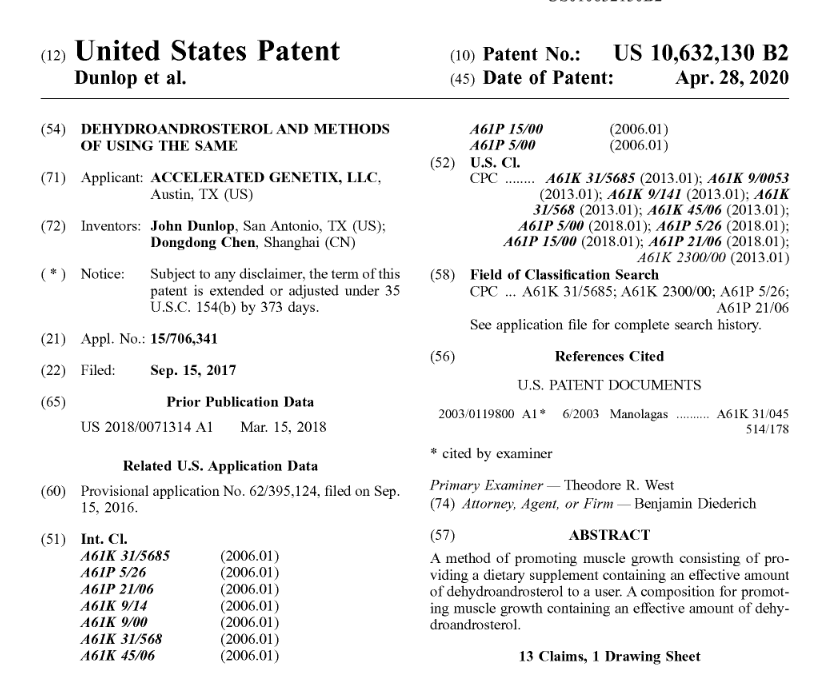
These guys should be writing romance novels. From the patent link above:
Animal Clinical Pre-Trial Evaluation
Caprine studies were also performed in two test animals. The test animals selected were monozygous male twins, castrated and placed in separate pens not later than six weeks after birth.
At approximately three months of age, one of these two goats was selected to receive daily DHA in a single, bolus, oral dose. The other goat was not given DHA, and served as the control. All parameters were equalized (pen size, ambient temperature, once daily exercise for 15 minutes on tread mill, 30 minute “play” time with other goats, twice daily ad-lib feeding of identical source feed, etc.)
Dosing was initiated in the test goat at 50 mg. After two weeks, the dose was increased to 100 mg, then after another two weeks increased to 200 mg, then maintained at that dose for an additional four weeks.
At the end of the eight week testing period, the two test animals were weighed to establish gains made from their original base-line weight at the beginning of the study.
Both goats began the study at 46 pounds. At the end of testing, the control goat weighed 61 pounds, indicating a 33% general weight gain. This was considered to be within the normal rate range of development as per the opinions of the experienced pen managers in charge of housing the goats. However, the DHA test goat’s weight increased from 46 to 73 pounds during the same test period, indicating a 59% general weight gain. The goat on the DHA regimen demonstrated greater appetite and food intake, and subsequently experienced weight gain approximately double that of the control goat. The weight gain of the test goat exceeded standards for statistical significance over the control, establishing a positive correlation between enhanced weight gain and DHA supplementation.
It had been anticipated that exogenously supplied androgen replacement, especially at higher doses, may reinstate typical, male behaviors such as bucking and mounting in castrate males. Alpha-male behavior was indeed noted to be established in the test goat when placed in the play pen with superior goats. This was manifest by the test goat challenging two larger goats with pre-established social hierarchy that were housed at the same facility.
Additionally, the pen manager in charge of the test goat noted another, unexpected observation, related to the behavioral demeanor of the animal. The test goat was observed to become unusually compliant and friendly toward all visiting humans and pen personnel. The pen manager mentioned that most goats protest the daily tread mill exercise in a predictable manner, and also tend to leave a portion of their daily food rations uneaten. However, the test goat became very “well behaved” once the dose reached 100-200 mg per day, happily engaging in forced exercise and eating all or more of the typically supplied rations.
It is unclear why DHA induced such pronounced behavioral improvement in the higher-dose caprine model, but, even at lower doses, supplementation demonstrates physical improvements in a trend similar to that noted by the human test subjects. It seems likely that the majority of weight gain associated with DHA use could be accounted for by lean muscle increase, based on the knowledge of DHA’s biological activity and the observations of its subjective results upon supplementation.
These guys may have George’s example beat.

3 Likes
I would agree with you on most compounds, but disagree in regards to Rad140. I put on a significant amount of muscle in far too short a period using this. Not advocating for people to go out and buy it, but I had a hell of a response on it.
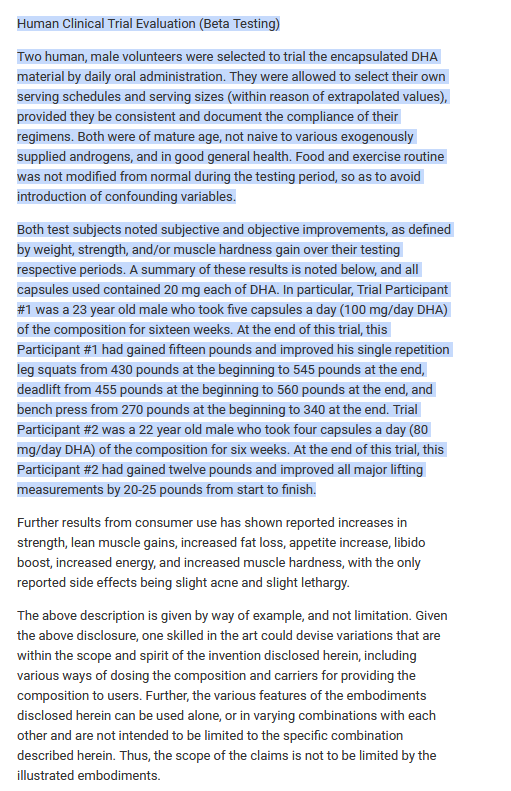
Was this peer reviewed by the same people that make the product? Either those are the most outstanding results ever recorded, or they are an outright lie. Most likely the latter.
1 Like
High School Science Fair level BS. B+ for creativity on the “animal clinical pre-trial”.

2 Likes
SARMs and Prohormones are technically different, but for clarity did you take rad140 orally from a supp shop or injectable?
2 Likes
It was an oral liquid from a supplement shop 30mg daily dose, and i split dosage e12h. I remember reading somewhere that better absorption was achieved if it was applied to the gums… Couldn’t tell you if that’s true or not (because you still had to ingest it after) but i had great results.
My gums sure AF weren’t happy about it though. Took a full on deep cleaning to undo the damage (would’ve paid more attention to brushing my teeth had i known)
1 Like
Well I won’t knock it if you say it works!
1 Like
Rad140 is s sarm not a prohormone. Sarms do work, they are the same as steroids.
2 Likes
Huh… i wonder who this could be…
Welcome back ![]()
3 Likes
The only effective PH still on the market in the USA is 1-dhea
Some online stores in Aus/europe (and real stores… though I think the last physical store selling these products in Aus was shut down) sell drugs like chlorodehydromethylandrosenediol, dehydromethylandrostenediol, methylepitiostanol, sarms etc.
Its a grey area as to whether its legal or not. In the USA I believe its illegal, but many online clear net stores still sell em… including ebay.
1 Like

Nonsteroidal SARMs: Alternative to Androgenic-Anabolic Steroids
Discovered in the late 1990s, SARMs are performance-enhancing agents that stimulate anabolism (i.e., increase muscle mass and strength) and facilitate recovery from exercise.9 SARMs are not anabolic steroids; rather, they are synthetic ligands that bind to androgen receptors (ARs).9 Depending on their chemical structure, they function as full agonists, partial agonists, or antagonists.9 Each SARM-AR complex possesses a different conformation, and various tissues (e.g., skeletal muscle, bone, prostate, brain, skin, liver) display a unique pattern of AR expression.9 It is, thus, in a tissue-selective manner that SARMs mediate coregulators and transcription factors or signaling cascade proteins to promote anabolic activity.10 Nonsteroidal SARMs serve as an attractive alternative to anabolic-androgenic steroids because they have fewer limitations.7 In contrast to steroidal androgen preparations, SARMs display high oral bioavailability.11 Nonsteroidal SARMs also exhibit diminished androgenic activity because they are not metabolized to dihydrotestosterone (DHT) by 5 alpha-reductase, an enzyme that is highly expressed in androgenic tissues.11 They are also not metabolized to estrogen by aromatase.11 For these features combined, nonsteroidal SARMs have been deemed to be advantageous over their steroidal counterparts.11 Indeed, SARMs have shown substantial therapeutic promise for male contraception and in the treatment of osteoporosis, prostate cancer, sexual dysfunction, benign prostatic hyperplasia, Alzheimer’s disease, muscular dystrophy, breast cancer, and muscle wasting associated with cachexia and sarcopenia.9 Fueled, at least in part, by the perception that SARMs are safer than anabolic steroids, recreational users are now leveraging the various anabolic profiles of different SARMs to selectively achieve results in terms of “bulking” and “cutting.”12,13 Bulking refers to a muscle-gaining phase that combines a weight-gain diet with intense weight training, whereas cutting refers to a fat-losing phase that combines adherence to a strict weight-loss diet with aerobic exercise and less-intense weight training. Anecdotal evidence claims that different SARMs yield different results in terms of bulking versus cutting, which is why bodybuilders and other fitness enthusiasts commonly use them in combination (or stacked ) with each other.12,13
Testolone/RAD-140
Testolone is a SARM used primarily for the treatment of muscle wasting and breast cancer. Developed by Radius Health, Inc., Testolone is reportedly still in first-stage clinical trials, with results expected later this year. Thus, little is currently known about its safety. One recent case report, however, describes significant liver injury in a 49-year-old man who had taken the drug (dose not reported).21 Elevations in bilirubin, AST, ALT, and creatinine indicated mixed hepatocellular-cholestatic liver injury. Liver histology also revealed inflammation. However, all liver tests had completely normalized at 12 months following his initial presentation. For gaining lean muscle mass and strength in the gym, SARMs users anecdotally recommended that Testolone be taken at 5 mg to 30 mg daily for 8 to 16 weeks.23 There is additional anecdotal evidence of side effects including sleeplessness and lethargy.24
Conclusion
SARMs are investigational drugs that have been studied for more than 20 years, yet none have received FDA approval, even for conditions in which the benefits might outweigh any significant risks. Much of the evidence regarding the performance-enhancing benefits and overall safety of SARMs is anecdotal rather than founded on scientific investigation. The few clinical investigations of SARMs have identified heart attack, stroke, and liver damage as potentially serious health risks. Individuals who are most likely to use SARMs recreationally include bodybuilders, fitness enthusiasts, and those with physically demanding jobs such as police officers and firefighters. In addition to what is available for purchase online, popular OTC products labeled as SARMs include SARM-X and Osta-Plex, which can currently be found at some nutritional supplement stores.
Pharmacists have an obligation to educate the public on the potential health risks associated with SARMs use. Pharmacists should recognize that individuals may not disclose all supplements used and should inquire about their use when it is pertinent. Even when a complete list of supplements is provided, users may be unaware of all the compounds that are actually contained within them.5,29 Pharmacists should caution individuals about supplement use, particularly when the source may be questionable, and help them understand that supplements are not regulated as prescription drugs are. When a person discloses a health issue, it is important for the pharmacist to have the proper knowledge to identify all possible causes. The pharmacist should especially consider the use of SARMs if an individual’s profile matches a group that typically uses performance-enhancing supplements and/or is experiencing adverse effects that are associated with SARMs use or PCT.
The content contained in this article is for informational purposes only. The content is not intended to be a substitute for professional advice. Reliance on any information provided in this article is solely at your own risk.
1 Like
I get your point. But that’s like saying Tamoxifen is the same as estradiol. SERMs and SARMs are acting on the same receptors but since they are structurally not steroids, the confirmation of the receptor ligand complex looks different. How it looks depends on the SARM. That’s the reason researchers are putting their hope into SARMs because they could find one that’s:
-
Tissue selective, for example only active in muscle tissue
-
Receptor selective, so only acting on some androgen receptors or responsive elements
-
Co activator / repressor selective which means acting on a receptor and ARE but having different gene transcription effects.
Up until now it’s difficult to say if there is one that actually has benefits. That’s why I get your point. As they also act on the same receptor and you still have to PCT. And they have similar side effects.
2 Likes
https://www.sciencedirect.com/science/article/abs/pii/S0039128X11000419
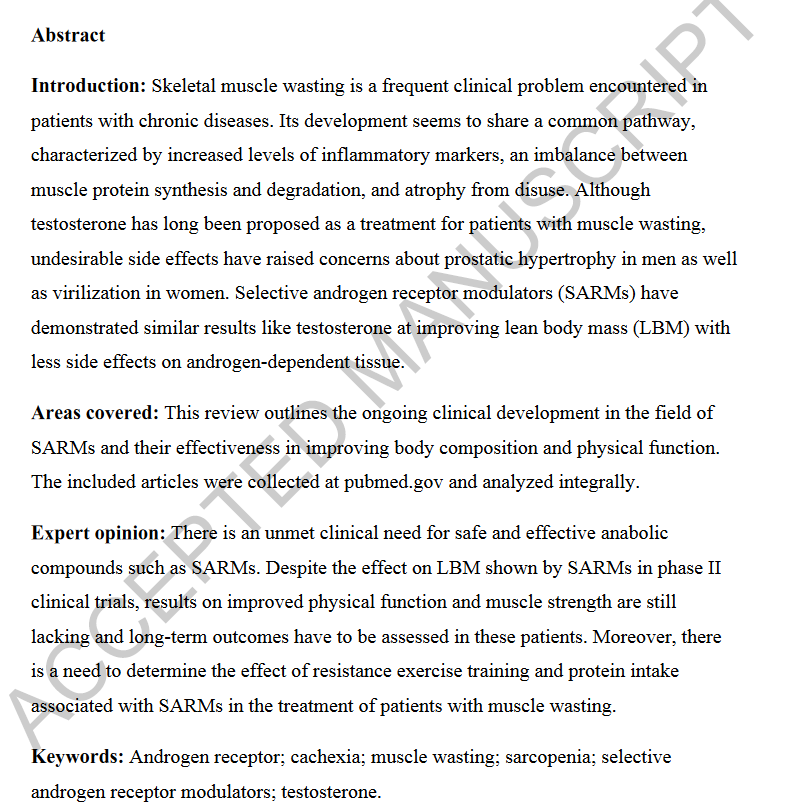
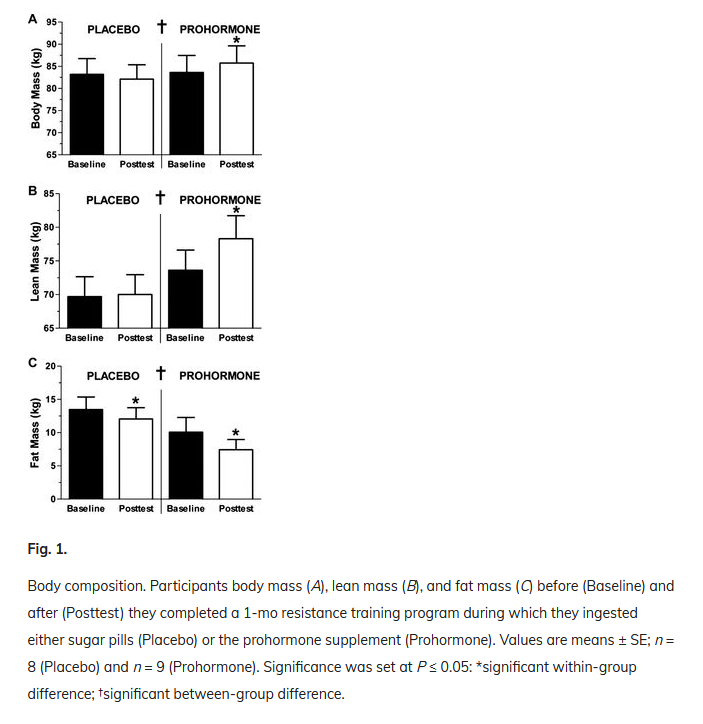
https://journals.physiology.org/doi/abs/10.1152/japplphysiol.00616.2013
Long story short, it works but as always be ready for the Faustian bargain. At least you are getting some sweet Gainz unlike 3-AD if you’ve got your training and diet in check. But those Gainz may be temporary and at the expense of your precious health.
So dumb question here…
Taking exogenous T will shut down your natural T levels, but also it takes some time for that to happen (>2months), according to the T-Replacement forum. So if one were to cycle T, or a SARM like RAD140 for a month, would natural T levels actually shut down during that timeframe or would they just diminish a bit?
I only ask because I cycled RAD140 for a month and never felt any overt symptoms of low T when I cycled off… I also didn’t lost any of the muscle I had put on (or at least not any appreciable amount), which leads me to believe that my natural T wasn’t shut down.
1 Like