Many members of this forum have been preaching “No AI to start with” long before Danny got here including myself. I’m surprised you are crediting Danny with this but he was the squeakiest wheel for awhile.
1 Like
I seem to remember the most prominent members were the biggest AI pushers.
One day I jumped in on a conversation and basically told Danny that I needed an AI because of high E2 symptoms. He patiently explained to me that I was probably sensitive to hormone fluctuations, and it wasn’t high E2 causing the symptoms. After a few discussions, he had convinced me to try the same way he stopped taking an AI, and I’ve never felt better, even with my “high E2”.
Basically, nobody else took the time to convince me like Danny did.
1 Like
It was definitely prominent in the KSman era when I first joined. It seemed by 2020 it was well known that AI was not needed to “start” a protocol. It has its place but most don’t need one with the proper dose. It took me over a year to figure that out for myself and I was going against the grain at the time. Here’s one from 2018… no AI recommendation
I’m not doubting that you and others were trying to get people to try TRT without an AI. But my problem was that I was convinced that I needed an AI. I pretty much ignored any posts saying otherwise. It wasn’t until Danny used pretty basic logic, which convinced me to give it a shot without an AI, that I actually opened up and listened to someone who I disagreed with.
1 Like
That is awesome. Now if he could use basic logic with TRT. I have received more data from another provider and have some follow up him. I will post that info and weave into treatment above.
But hey we are getting somewhere. Danny and I agree the long term impact of fT 80-150 ng/dl is unknown. It is a start and by logical extension the long term effects of running above human physiology are also unknown and most likely a nonlinear function of deviation from physiologic range.
Hence, he should also caution the ignorant looking for relief about the risk of 30 to 50 ng/dl and not just above 80 ng/dl. Yields a false sense of security.
He did. That’s exactly what he did. That’s why I stopped poisoning myself with anastrozole.
TRT as in the use of exogenous T to replace endogenous hypo levels back to levels found in eugonadal male.
That would be reasonable standard of care consistent with four pillars of medical ethics. Normalizing that many are running 30 to 50 ng/dl for symptom relief is not. Informed consent seems in order and looking out for the most vulnerable.
My main problem with Danny is too much passiveness over E2. Ratios sound good in theory but I don’t believe they exist. I myself now am trying new things and ok let’s drop the AI, but then I do absolutely believe I have to reduce dose. He was just too nonchalant about going higher and higher and “letting it work itself out, higher e2 comes with higher T”. At some point it doesn’t matter some level of E2 is a cut off for certain people.
This is the result when run your T levels higher than that found in 99.999% of young, eugondal males and remove any AI use.
By the way still really really early. I am feeling weird, I feel less wired physically. At the same time I am over come with more emotions I have to juggle, I guess it comes with E2 as it goes back to baseline on 100mg and no AI.
But no way in hell can I inject more and more T without AI like its all good.
1 Like
Example from the 1970s:
Circadian TT fluctuation…
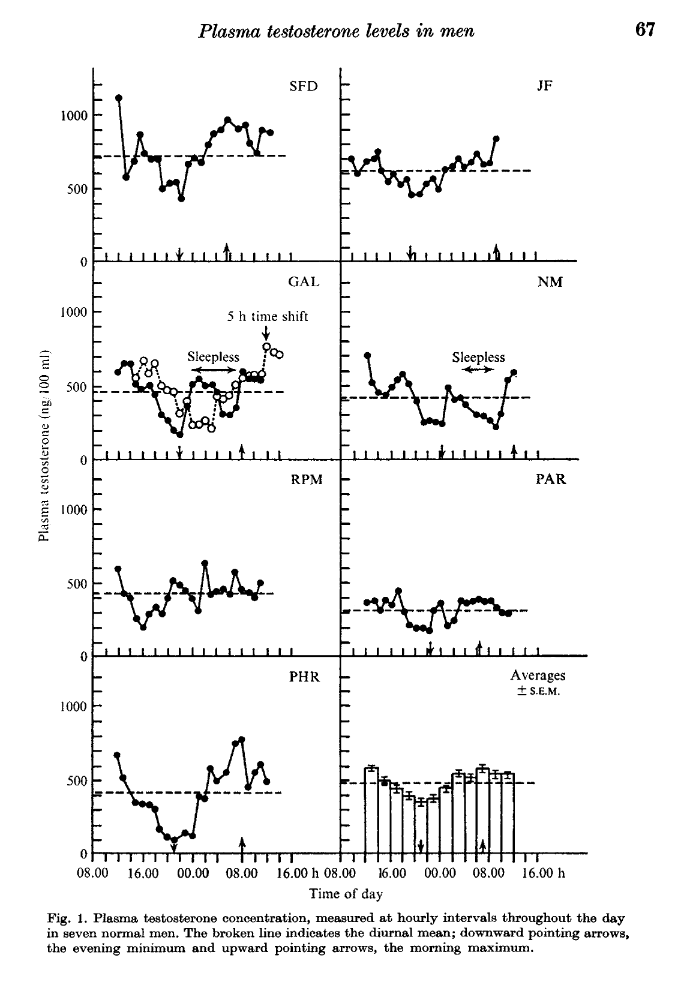
Notice subject SFD. He is at the “pinnacle of manliness”, when men were men in terms of TT levels.
Here’s his daily variation with respect to max TT every day…
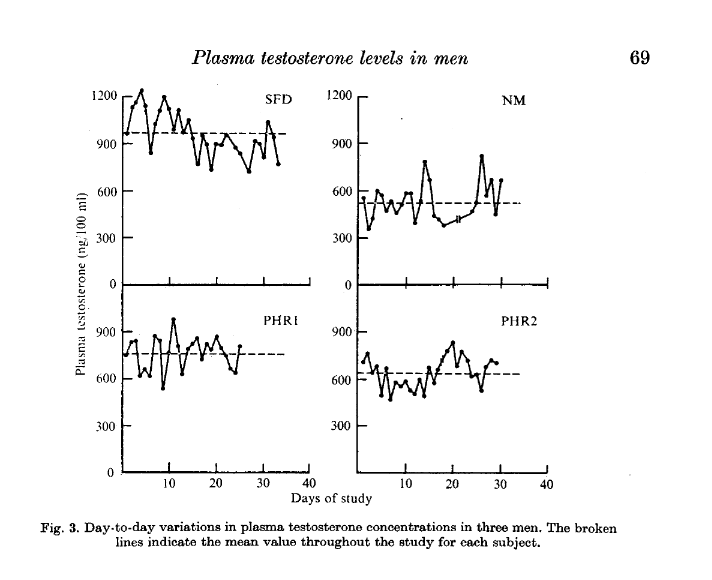
Notice anything strange?
Yes, correct. SFD’s INTRADAY PEAK is what many today have for a WEEKLY TROUGH (200-250 mg/week TC E7D):

Danny and TOT World either don’t get it or purposely misleading people.
Eugonadal guys always in the green shaded region. TOT Land many times may only touch the ceiling of the green shaded region.
2 Likes
…
[quote=“tareload, post:1, topic:277585”]
TLDR (great suggestion by @kazuya_mishima1):
Danny and the TOT folks are mistaken to put it politely with respect to pharmacokinetics and dose response of injectable exogeneous testosterone. They act like it’s some mystery how you will respond to injectable testosterone. It really isn’t and we can put a very confident estimate on it. Many guys running TOT protocols (150+ mg/week) are way above physiologic levels all week long 24 hours a day. Read on if you’d like to understand with an example in excruciating detail. Pay attention to numbers thrown out there. Are they peak or trough? Learn the basics of pharmacokinetics so you can inform yourself about TOT World before you go that route. Then at least you can give informed consent before you embark on their large uncontrolled science experiment that they themselves will admit has an uncertain long term result.
BEGIN:
I reached way back for you guys. 1970s-1980s back when we had REAL men.
Don’t say I never gave you anything:




Check out subject III

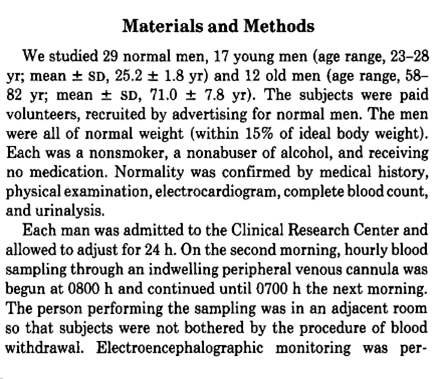
TEMPORAL VARIATIONS OF TESTOSTERONE LEVELS IN THE PERIPHERAL BLOOD PLASMA OF MEN

Look at subject SFD…
daily variation of the max TT levels…

Now let’s go back to this plot:

Where do you think these numbers come from? They represent values measured in a sample of men that can’t be higher than their peak intraday value . So either it’s the max TT or < max TT level these guys are hitting in a day. There’s is almost no one walking the face of the earth “unassisted” with peak ( much less mean ) daily TT levels above 1200 ng/dl.
After you let that sink in then come back to this:
Be careful to clarify where the “1000” is in the context of treatment. Trough or peak?
Corrected for testosterone amount in the ester, of course you can . A human doesn’t eliminate free endogenous testosterone any different than they would eliminate free exogenously introduced testosterone.
Ask yourself, what is being referred to here? Danny gets 1000 ng/dl where on 250 mg/week of test ester? Peak/trough?
The answer would be trough. What would Danny’s peak TT and mean TT be if he is getting a trough of 1000 ng/dl? Assume E7D or E3.5D injection.
1 Like
Wtf is TOT?
Yeah that’s crazy to me.
I think lab ranges are typically 2 standard deviations on each side of the mean, so if we take the typical 9-25ng/dL Free T range, that gives us a mean of 17ng/dL and SD of 4ng/dL.
Free T at 33ng/dL would be 4 standard deviations above the mean. Very high but not completely insane at around 1 in 1000 men with those levels.
Free T at 80ng/dL however would be almost 16 standard deviations above the mean.
Personally I don’t really care about the semantics of TRT vs TOT vs cruising vs blasting, etc…people can define their own priorities. But at some point you have to use common sense, and if you’re hoping to get away with cruising where 1 in 10000…(58 zeros) men theoretically have their Free T, you’re probably in for a bad surprise
4 Likes
“I’ll take 8 to 16 Sigma Testosterone Therapy for the win, Bob.” ![]()
#8-16STT4THEWIN
Make sure to check what it is you will be winning though.
Thanks for your thoughts @disciplined_trt. Great points.
2 Likes
Haha.
I was thinking about how I’d try to explain to someone how absurd 16 SD’s is. And you can’t really because those numbers are ridiculous, but I think I’d go with…
“Ok, let’s say we have 10 billion people on the planet. Now imagine there’s 10 billion times those 10 billion people. Really think about it; it’s not 10, 100 or even 1000 times those 10 billion people, it’s 10 billion times those 10 billion people. Right? Ok…now take 10 billion times that population, so that you have 10 billion times 10 billion times those 10 billion people. Now do that again and again and again, so that you end up with a population of 10 billion times 10 billion times 10 billion times 10 billion times 10 billion times the current population of 10 billion people we have. Ok? Now out of that population, there is statistically one guy with Free T at 80ng/dL”
4 Likes
Again, comparing apples to oranges.
What do you mean? Which comparison doesn’t make sense to you?
my emphasis on the [sic]
1 Like
I think Danny is doing everyday subq, at least currently.
It is interesting though, i dont know if his receptor resistance theory is all bullshit, as i now guys who get no benefit from a low dose for some reason. It would be pretty odd if the same person could feel good on 70mg or 300mg per week.