If you scroll up that’s exactly what I said the only info I left out was what size vial…it’s 1ml of 200mg of cyp and I take .5cc just like you said every 5 days which your right it’s 140mg a week or 200mg every 10days…I know exactly what I’m taking…that’s not what I asked…the syringe I use is 3cc and if I’m told to pin eod I’ve never done that and I’m not the best at reading a syringe so was just asking what mark is best it just seems like I’d only draw a little bit of cyp eod and maybe a 3cc syringe is to big…nothing I said was incompetent and never said I didn’t know what I was taking
It seems when I go to the doc they wanna all talk about taking clomid and send me on a roller coaster ride with different regiments so I turn to y’all for advice and I’m slowly learning…I’ve only ever done IM because the docs say that’s the only way to do it. I use a 23 gauge to draw and a 25gauge to pin 1”
1/2" ones should in the rightarea
Man does private md mean I have to draw my own blood? Ahhh seems sketchy
You could always try sub q. Much easier
Sorry I pin in the thigh about a hand length from my knee. Can a 1/2” insulin syringe hit muscle in that spot or would I do different
No dude you go to Lab Corp.
So you are pinning 0.7 cc a week, or 0.1 a day. EOD would be 0.2. Sub-Q works better for some guys, it works exactly the same for others, it results in increased E2 for others. I do sub-Q. 1/2 pis will hit muscle in a low fat area.Id it doesn’t, it’s just a sub-Q pin. No harm no foul. Most of us are using 27 ga or 28 ga I believe. I have 27 ga insulin needles.
Should work fine. Either way it’s still getting absorbed. Fat or muscle. I go around my naval, its pain free and no pip
Hahaha phew lol ok no doubt thanks
1 Like
Perfect thank you so much that helps a lot, what size insulin needles and do you back fill them or draw it out?
I back fill with a 3 mL harpoon that comes in the box with my amp. It’s a lot faster than drawing with a little needle and is actually safer. Little things like bits of rubber stopper that get into a draw needle won’t pass through the finer needle into you.
I’m using 27 ga 1/2" usually, for sub-Q. I would lean towards a 1" for IM if I really wanted IM.
1 Like


Here is my total blood work from my yearly right before I started an ai this is when I first realized cholesterol was messed up
Ok great so I think my first step is lower my ai dose. I’ll then get my sbgh tested along with my insulin and glucose. I’ll wait a month? Then test again and post my labs. If still messed up I’ll start doing my dose of cyp more frequent. Think that’s a good start or just change up everything right away? Are my labs that off with exception of to low of estrodial?
Sick care doctors were taught in medical school TRT causes prostate cancer and the medical community has a very negative view on TRT, add to the fact doctor are the conduit for big pharma where profit is driven by patented drugs and you understand why hormones which aren’t patented are rarely used in sick care.
Sick care doesn’t even have a doctor that specializes in TRT, above explains why.
1 Like
Your percentage of free testosterone is 3.2. Your SHBG is low, likely very low. Ideal range is 2-3%. High SHBG guys can be as low as 0.5%, binding a large amount of their testosterone. I would be fine with your testosterone status and current dosing schedule. I would consider reducing, even eliminating, the aromatase inhibitor. That may be tough with SHBG so low.
I would also take a look at thyroid levels.
2 Likes
Your cholesterol is not bad. Your triglycerides are high, which may be genetic. Your HDL’s are low. Get some Omega 3’s, like fish oil, olive oil, flax oil, that kind of thing (or just Omega 3 caps) and your HDL’s will come up and your ratio will be okay. SHBG is a good test to run, pretty much whenever, so that you know what you are currently dealing with.
1 Like
Was this lab the one that had you prescribed an AI? The reason I ask is the only estrogen lab I see there is estrogen total which isnt a good one to go off of. So you may have never needed an AI in the first place if it was based off this lab. The one in your first post looks like the correct one though.
Well his estradiol is 23, but it is a non-sensitive so it is probably much lower.
We can also assume his E is low because of his disproportionate free T to TT.
SHBG and estradiol usually go up and down together, this is why anastrozole increases free T so much.
1 Like
Probably not.







The ECLIA test (aka immunoassay or IA) for E2 management is commonly used for those on TRT. It is not an incorrect test or a test for women, but simply one way to check estradiol levels. The other commonly utilized test is the LC/MS/MS method (aka liquid chromatography dual mass spectrometry, sensitive or ultrasensitive). It is the more expensive of the two. There are inherent advantages and disadvantages to each of these two methods. I have been fortunate to be able to speak with professionals who work with both methods. One is a PhD researcher for Pfizer and the other is a medical doctor at Quest. I’ll summarize their comments.
The ECLIA method is the more reliable of the two in terms of consistent results. The equipment is easier to operate thus accuracy is less reliant on the skill of the operator. If the same sample were to be tested twenty times, there would be very little, if any, difference in the results.
The ECLIA method is not as “sensitive” in that it will not pick up E2 levels below 15pg/mL. If your E2 level with this test is 1-14pg/mL, the reported result will be “<15”. Because of this, it is not recommended for menopausal women, men in whom very low levels of E2 are suspected, or children. In other words, if your levels are below 15pg/mL, and it is important to know if the level is 1 or 14pg/mL, you do not want this test. For us, this is likely moot, since if you are experiencing low E2 symptoms and your test comes back at <15, you have your answer. For a woman being treated with anti-estrogen therapy for breast cancer, it may be necessary to know if the E2 level is zero or fourteen because therapeutically, they want zero estrogen.
A disadvantage to IA testing is that it may pick up other steroid metabolites, which in men would be very low levels, but still could alter the result. Another potential disadvantage is that elevated levels of C-reactive protein (CRP) may elevate the result. CRP is elevated in serious infections, cancer, auto-immune diseases, like rheumatoid arthritis and other rheumatoid diseases, cardiovascular disease and morbid obesity. Even birth control pills could increase CRP. A normal CRP level is 0-5 to 10mg/L. In the referenced illnesses, CRP can go over 100, or even over 200mg/L. Unless battling one of these serious conditions, CRP interference is unlikely.
The LC/MS/MS method will pick up lower E2 levels and would be indicated in menopausal women and some men if very low E2 levels are suspected and it is desired to know exactly how low, children and the previously mentioned women on anti-estrogen therapy. It will not be influenced by elevated CRP levels or other steroid metabolites.
While some may believe the ECLIA test is for women, on the contrary, as it pertains to women on anti-estrogen therapy, such as breast cancer patients, the LC/MS/MS is the test for women as CRP levels are a consideration and it is necessary to know if the treatment has achieved an estrogen level of zero.
On the other side of the coin, LC/MS/MS equipment is “temperamental” (as stated by the PhD who operates both) and results are more likely to be inconsistent. Because of this, researchers will often run the same sample multiple times.
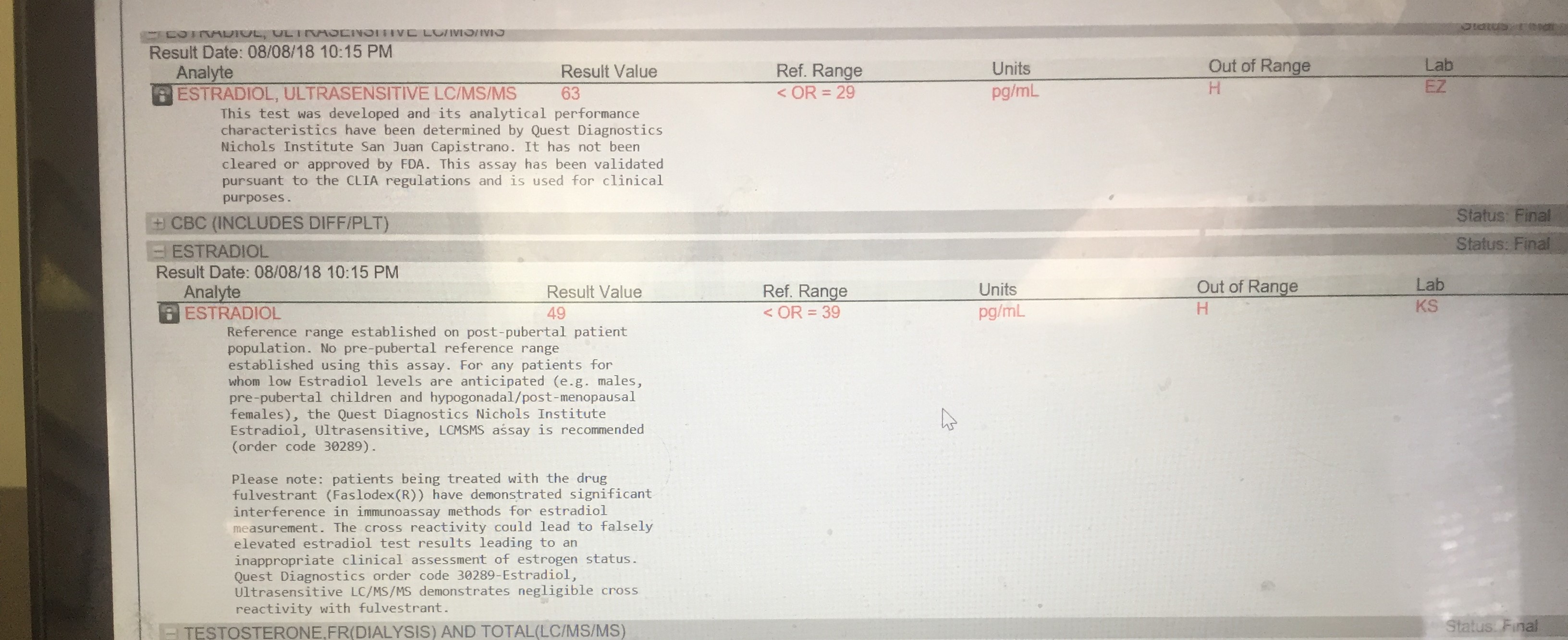
It is not clear if FDA approval is significant, but this appears on Quest’s lab reports: This test was developed, and its analytical performance characteristics have been determined by Quest Diagnostics Nichols Institute San Juan Capistrano. It has not been cleared or approved by FDA. This assay has been validated pursuant to the CLIA regulations and is used for clinical purposes. This statement is on LabCorp’s results: This test was developed and its performance characteristics determined by LabCorp. It has not been cleared by the Food and Drug Administration.
It is unlikely that any difference in the same sample run through both methods will be clinically significant. Estradiol must be evaluated, and it should be checked initially and ongoing after starting TRT. It obviously makes sense to use the same method throughout. Most important are previous history and symptoms related to low or high E2. Those are correlated with before and after lab results. Any estradiol management should not be utilized without symptoms confirmed by lab results.