New doc requesting bloodwork:
Comprehensive Metabolic Panel
CBC
Lipid Panel
Testosterone Free and Total Estradiol Sensitive DHEA-S
TSH
PSA
LH
SEX HORMONE BINDING GOBULINE
Labs will be done at Labcorp
Any additional tests I should have done
New doc requesting bloodwork:
Comprehensive Metabolic Panel
CBC
Lipid Panel
Testosterone Free and Total Estradiol Sensitive DHEA-S
TSH
PSA
LH
SEX HORMONE BINDING GOBULINE
Labs will be done at Labcorp
Any additional tests I should have done
@KSman
Just found your sticky on bloodwork.
Labs to be done before you start TRT
-LH and FSH [LH/FSH]
-TT
-FT or bio-T
-E2
-Prolactin [optional in most cases]
-DHT [sort of a waist of time and blood if your testosterone levels are low]
-PSA
-DRE: the dreaded digital rectal exam, doc gives you the finger.
Labs to be done when on TRT
-TT
-FT or bio-T
-Implications of injections VS transdermals [and injection frequency]
-E2
-Prolactin [optional and almost never on-going]
-DHT [should be checked, but perhaps not on-going]
-LH/FSH [optional and one last time -do I have cancer?]
-PSA
-DRE: the dreaded digital rectal exam [Your doc does not enjoy this either!]
Labs to never do and timing issues:
-DO NOT test E2 ultra sensitive
-DO NOT do saliva testing for T or E2 and expect any help here
-DO NOT test for free E2
-DO NOT test total estrogens
-DO NOT test PSA within 48 hours after a DRE [digital rectal (prostate) exam] or ejaculation
-DO NOT test prolactin with 48 hours of orgasm, avoid hugging puppies and babies
-DO NOT do lab work when muscles are sore from training or injury as your “liver markers” will show high levels. Those “liver tests” are really not liver specific.
-DO NOT waist time and money on tests that you cannot take any action on. Example, testing IGF-1 for growth hormone status if there is no way you could every pay for GH or actually legally qualify for GH.
-DO NOT routinely test for LH/FSH when on TRT, perhaps once to rule out certain testicular cancers and never again
-DO NOT test for serum DHEA, must test DHEA-S
-DO NOT do saliva testing for T, DHT, DHEA, pregnenolone if taking sublingual/buccal T, pregnenolone OR DHEA OR other steroid. The tests will be wrong and you do not want cross reactivity unknowns
-Testing E2&TT&FT makes also testing SHBG sort of useless.
Labs that are stupid after you start TRT
-LH/FSH
Thyroid labs [basic first line]
-TSH
-T3 no see fT3
-T4 no see fT4
-are you getting enough iodine? probably not! KSMan? - Testosterone Replacement - Forums - T Nation
-? stuff that Hardasnails will suggest to me via PM
Thyroid symptoms [hypothyroidism or subclinical] Dry Skin, sparse outer eyebrows [observe others], feel cold easily, low body temperatures, general non-pattern hair loss, enlarged, lumpy, sore or asymmetrical thyroid gland. Many symptoms are the same as low-T.
Adrenal labs
-Cortisol four sample saliva testing [the gold standard]
-Pregnenolone [the foundation of the adrenal hormones and all steroid hormones *]
-DHEA [can’t make T without it] no see DHEA-S
-DHEA-S [DHEA Sulphate]
Vit-D is multi-step derived from cholesterol directly, not via pregnenolone. Pregnenolone is also direct from cholesterol. Cholesterol is really the root of all steroid hormones. [Because cholesterol can be considered a precursor of testosterone, and testosterone a metabolite of cholesterol under Federal Statute [http://www.justice.gov/dea/pubs/csa/802.htm], cholesterol is technically a schedule III controlled substance and is subject to criminal penalties as an illegal anabolic steroid. Attempts by John McCain and others to explicitly classify DHEA as a schedule III anabolic steroid have nonetheless failed. See http://frwebgate.access.gpo.gov/cgi-bin/getdoc.cgi?dbname=110_cong_bills&docid=f:s762is.txt.pdf13 ]
General health labs
-CBC: Complete Blood Counts
-Hematocrit: Part of CBC but needs its own discussion
-Lipids: Fasting Cholesterol and related
-Vit_D25 hormone -yes vitamin D becomes an essential steroid hormone
-Glucose: Fasting levels indicate insulin function
-Liver markers -are they really liver specific? [Hint: not]
Things that you can determine without lab work
Symptoms: Why are you here
-Brain fog, no one knows what that means but everyone knows if they have it!
-Social withdrawal - “I would rather not go out”
-Why do I have boobs? This really is depressing if prolactin is the cause!
-Why do I carry fat like a woman?
-Why am I a moody bitch?
-Can’t get it up?
-It is up, now it’s gone.
-My penis is numb -your nerves love T too. Things to do with testosterone cream.
-My testes are softer and smaller
-My testes ache 24x7
-My scrotum is up-tight, gives “how are they hanging” a whole new meaning.
-Nocturnal erections -necessary but not sufficient
-“morning wood” -things are working
-Why do really hot looking women and girls now look like art instead of lust?
-I felt great when I started TRT, where did that go? Neural transmitters rule your life.
-My TRT seems ineffective or never was. Things that crash in the night.
-On TRT and still do not feel right, something else is wrong.
-Loss of hair on lower legs, skin below the knees is smooth and shiny.
-Why do I feel cold easily or all of the time?
-Why do really stressful situations leave me feeling physically beat up. Adrenal fatigue.
-Dry skin, brittle hair and nails
-Skin on the back of hand is thin, crinkly. Pinched skin does not recover
-Gum disease, the ugly killer
-Why do I have a chronic cough [when taking a statin drug]
-I have visual field disturbances such as reduced peripheral vision
-My joints have started to ache
-TRT and now leg cramps
-TRT and wife says I am snoring more
-I am not depressed, I just don’t care about anything, no joy, no motivation, no reward
-I want sex twice a day and my wife/GF is freaking out. What do do about her.
-We fixed my wife’s hormones and I can’t keep up with her needs. [Give me her phone number!]
-I want sex twice a day and my wife/GF loves it. Why are you still here?
Related:
-pituitary MRI for younger cases of hypothyroidism “what is in there”
-testicular ultrasound exam, detects cancer [please help with other uses]
Serum E2 testing:
E2 is estradiol - in case you were wondering [E1=estrONE, E2=estraDIol, E3=esTRIol]. There are different lab tests to choose from and docs often get this wrong. Some testes have limited reporting ranges and will not report actual values below a certain level and might report <17 pg/ml instead of the actual value. The reason for this is that these tests were developed for work on women’s hormones. Women who are fertile have very high levels of estrogen and some tests are appropriate for those levels. Women who are post menopausal have low levels of estrogens and the need tests that are sensitive for those low levels. For post menopausal women with breast cancer, SERM drugs are used to push there already low estrogen levels even lower. Ultra sensitive tests are used to detect these very low levels to determine the effectiveness of the treatment.
For TRT, use the basic LabCorp serum E2 test or Quest Sensitive 4021x. DO NOT USE Quest ULTRASENTIVE! There are some similar issues with other testing labs as well.
DO NOT test for free estradiol
DO NOT test for total estrogens
DO NOT do Saliva testing, simply because very few people know what to do with that data.
Note that many older men, getting fat with low testosterone, can have more estrogen than their post menopausal wives! And old men and women can end up having similar body shapes.
E2 levels are modulated with low doses of aromatase inhibitors such as Arimidex/anastrozole. Optimal level is near serum E2=22pg/ml. Some doctors will prescribe 1mg/day which is a TOTAL disaster unless you are female and have estrogen positive breast cancer. Another idiot doctor mistake.
See this thread concerning problems with Labquest FT testing:
Note that Labquest can also report FT ranges that are about 5 times higher than reality. So you cannot compare Labquest results to Labcorp and others. FT lab results must be reported with lab ranges.
created
Apr '15
last reply
76
replies
KSman
Jun '10
Purechance contributed this:
[KSman says: Some of this testing may not be needed, some judgment is needed. Some docs will not do this because of HMO restrictions. Otherwise some insurance may not pay. Note that lab tests can run into a large amount of money if out-of-pocket. Labs that are used for routine followup of HRT treatment may need to be more focused from a cost-benefit point of view.]
Vitamin D deficiency is under-reported. A lot of people would benefit from a Vitamin D supplement.
GET the actual test results from the doctor’s office. DO NOT accept “oh, your test results came back fine or within range”. You are a paying customer. Make them fax you the results or get a new doctor, or ask for the results to be transferred, then get them from your new doctor.
You are the customer and have a say on what tests are run and your treatment plan. If you have a doctor that won’t work with you, find another one.
Doctors surprisingly know very little. You know your body better then they do. Insist on getting your symptoms treated.
Never just accept that “your results are normal.” Most doctors don’t know what normal is. Get your own results and do your own research. Always insist on seeing your actual results. Get a copy for your records (in case you are like most people here who have to go from doctor to doctor until they can find one who will work with them.)
DO NOT believe the ranges the lab report shows. Do your own research.
Here is some of what I have asked for or doctors have recommended:
Chemistry Panel (Metabolic panel with lipids)
Complete Blood Count (CBC)
Free Testosterone
Total Testosterone (<500 is not good. 700-1000 is good)
DHEA-S - Sulfate (low DHEA = increased risk of cardio complications + DHEA converts to T)
Prostate-Specific Antigen (PSA)
Estradiol
Homocysteine
C-reactive protein (High sensitivity) - (high = cardio risk)
TSH (Thyroid Stimulating Hormone) - not that important. It is inaccurate and too many doctors use it as the holy grail; T4/T3 numbers are more important.
[KSman says: All of the group above can be had as a male lab panel from lef.org, the price is right, but it is always out-of-pocket and insurance will not cover.]
Total T4
Free T4
Total T3
Free T3
Reverse T3 (excess T4 converts to RT3. High RT3 blocks free T3 - so your TSH and T3 numbers could look great, but are blocked by RT3 and you feel like @$#!)
Thyroglobulin Antibodies
Thyroid Peroxidase
Cortisol (low cortisol = low overall cellular functions)
LH (low LH = pituitary disfunction causing hypogonadism - need MRI to check for pituitary tumor)
FSH (same as above)
DHT (Dihydrotestosterone)
SHBG
IGF-1 (Insulin-Like Growth Factor) (indicator of Human Growth Hormone <200 = not great)
Prolactin
Progesterone
Pregnenolone (precursor of Cortisol, DHEA, and Progesterone + Preg resolves brain fog and improved memory)
VITAMIN B12
Vitamin D, 25-OH Total (should be 70-100 I think - almost everyone is deficient)
Vitamin D, 25-OH D3
Ferritin (critical for cellular function - low ferritin = low transport capability of hormones, etc.)
Iron, Total Binding Capacity
Iron, Binding Capacity
Magnesium, RBC (is important for cellular energy (ATP) production)
2 months later
TysonKilpatrick
Sep '10
KSman,
Although some of the symptoms you listed above have implied causes that are inferrible to a majority of your readers, it would be beneficial if you could give the possible relationship between the suspected pathologies which may result in these symptoms.
i.e. Can’t get it up. (possibly low or high E2)
Thanks
PureChance
Sep '10
Here is another consolidated comprehensive list posted by JanSz on another forum.
1 Metabolic Panel (14), Comprehensive
2 CBC w/ diff/PLT
3 VAP TM Cholesterol Test
4 Selenium, Whole Blood
5 Copper, serum
6 Zinc
7 Magnesium, serum
8 Magnesium, RBC
9 Potassium, RBC
10 C-Reactive Protein (CRP), Highly Sensitive, CSF
11 Fibrinogen
12 Homocysteine, cardio
13 Lipoprotein (A) Lp(A)
14 Iron and Iron Binding Capacity
15 Iron, Total
16 Ferritin
17 Transferrin
18 Folate, RBC & Hematocrit
19 Hemoglobin A1c
20 Hemoglobin, Plasma
21 VITAMIN A, E, B3, B12
22 Vitamin D, 25Hydroxy
23 T3, Total
24 T4, Total
25 T3, Free
26 T4, Free
27 T3, Reverse
28 Ultrasensitive TSH
29 Thyroid Peroxidase and Thyroglobulin Antibodies
30 Thyroglobulin
31 Thyroxine binding globulin
32 T3 Uptake
33 Prealbumin/Transthyretin
34 Insulin, serum
35 IGF Binding protein3
36 IGF-1
37 DHEA Sulfate
38 Aldosterone
39 Renin Activity, Plasma
40 ACTH, Plasma
41 Cortisol Binding Globulin (Transcortin)
42 7:30AM/12PM/3:30PMCortisol, Free and Total
43 Prolactin
44 Progesterone
45 Pregnenolone
46 Androstenedione
47 Estradiol, sensitive 140244 (370)
48 Estrone, Serum
49 Total Testosterone
50 SHBG
51 Albumin
52 Dihydrotestosterone
53 3aAndrostanediol Glucuronide
54 Ceruloplasmin
55 Coenzyme Q10
244.9 257.2 780.79
250.00 272.4 788.41
250.01 601.9 253.3
255.4 780.4 255.8
783.9
Helper
Sep '10
I’m finding this to be very overwhelming.
Is it possible to make a ‘TRT for Dummies’, and if this is it, then to make a ‘TRT for Retards’? Maybe have the abbreviations/terms explained, or with an explanation if you browse your curser over the term?
If I read this correctly, there are six (6) necessary labs to be done before TRT:
And, there are seven (7) necessary for after you have started TRT
TT (again)
FT (again)
Implications of injections VS transdermals (that’s a lab?)
E2 (again)
DHT
PSA (again)
DRE (again)
Labs to never do and timing issues:
…
-DO NOT test for serum DHEA, must test DHEA-S
If I MUST test for DHEA-S, why isn’t that in the ‘Labs to be done before’ or ‘Labs to be done after’ lists?
Also,
Labs that are stupid after you start TRT
-LH/FSH
Thyroid labs [basic first line]
-TSH
-T3 no see fT3
-T4 no see fT4
-are you getting enough iodine? probably not!
-? stuff that Hardasnails will suggest to me via PM
Adrenal labs
-Cortisol four sample saliva testing [the gold standard]
-Pregnenolone [the foundation of the adrenal hormones and all steroid hormones *]
-DHEA [can't make T without it] no see DHEA-S
-DHEA-S [DHEA Sulphate]
Does that mean that thyroid labs and adrenal labs are ‘stupid to do after you start TRT’?
If they’re important, should they be in the ‘labs to be done when you start’ list or ‘labs to be done when you’re on TRT’ list?
Are the General health labs important, and if so, should they be in ‘labs to be done before’ or ‘labs to be done after’ list?
I’m sorry if this post makes me sound like a jackass or like I’m being picky, but I really just don’t understand.
KSman
Sep '10
You do not test LH or FSH when on TRT as you will be shutdown and they will be close to zero. That is in the stickies.
Yes, general labs are important, and basic, too basic to make take up space here.
I did state “-LH/FSH [optional and one last time -do I have cancer?]” If FSH stays high with HPTA shutdown, you probably have a FSH producing testicular cancer.
Some say to test for thyroid and adrenal issues because if they are low, when you increase metabolism with TRT, you will find the next weak links, aka hitting the wall. The rest of answer it self evident. This issue is discussed many times in posts.
Was not saying when to test DHEA-S. You can do that any time you want and DHEA is also part of adrenal function. If DHEA is low, take some and test later to see if you need more or less. I did not state that you MUST test DHEA, only that if you do, test for DHEA-S, not DHEA. DHEA tests are quite useless for reasons that I will not explain now as I have stated the reasons many times elsewhere.
You two need to learn to learn and read between the lines. Asking to explain everything that you do not know it a bit much.
This sticky is not a TRT guide.
Use Google, there is a lot to learn. If I explained ever little thing the message would be lost. No one else has these issues. Please do not mess up this sticky with more questions like this, and this is not a place for a discussion about this.
Don’t ask me to explain all that I know about pathologies. This sticky is an attempt to create list of thing that you should consider and understand. And there are hints for you to follow. You need to study to understand.
Read other stickies and posts and search the web. If you cannot contribute to the knowledge here, do not post here in this sticky.
orangeblood
Sep '10
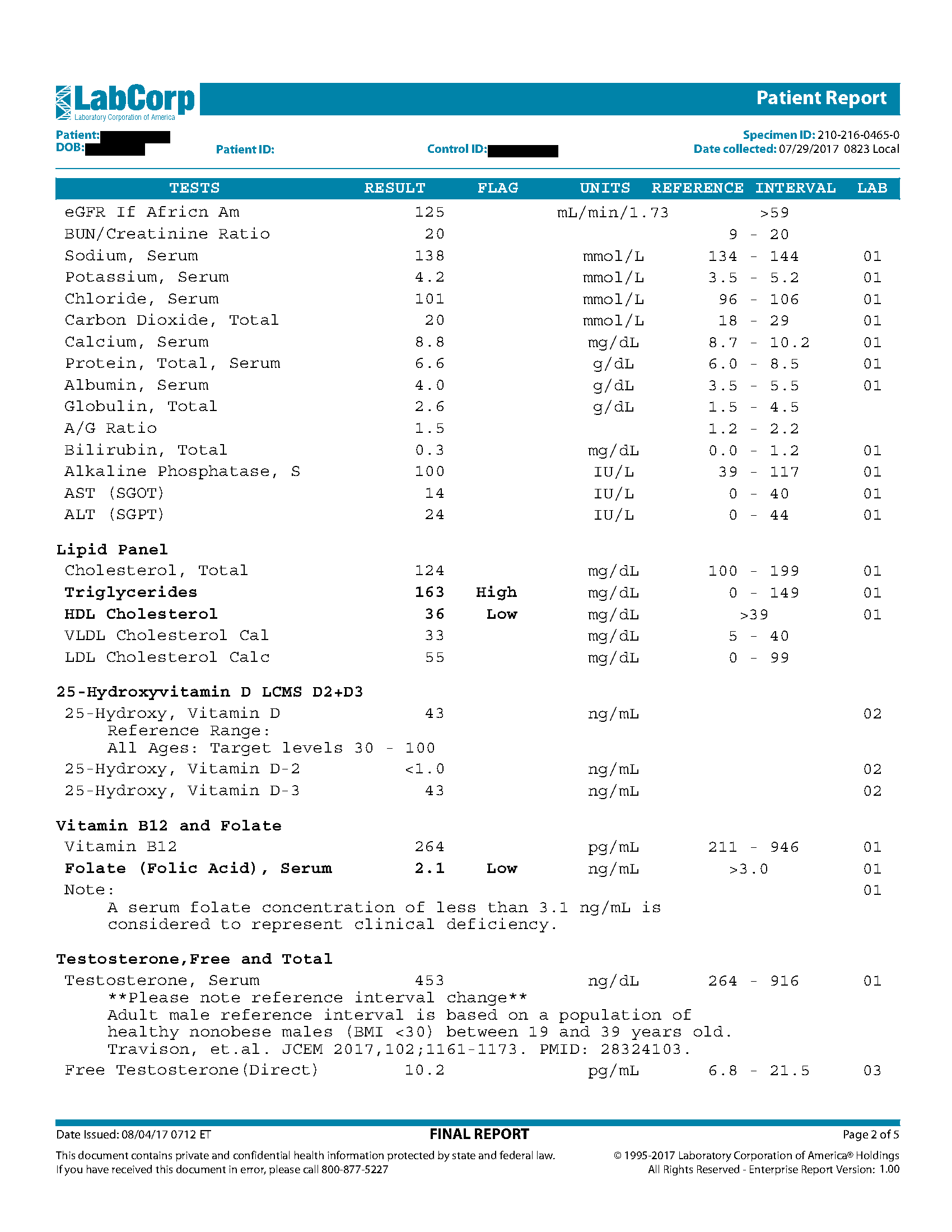
I had blood drawn this morning, hoping to have results by Monday.
Here is list with Labcorp codes:
Comprehensive Metabolic Panel 322000
CBC ????
Lipid Panel 303756
Testosterone Free and Total 140103
Estradiol Sensitive 140244
Estradiol 004515
DHEA-S 004020
TSH, FT3, FT4 004259,010389,001974
PSA 010322
LH / FSH 004283 ,004309
SEX HORMONE BINDING GOBULINE 082016
Vitamin D, 25-Hydroxy 504115 D2+D3 Fractionated, LC/MS-MS
Progesterone 004317
DHT 500142
Prolactin 004465
B-12/folate serum 000810
Wow, your case is fascinating and those are the most extensive series of blood tests I have ever seen!
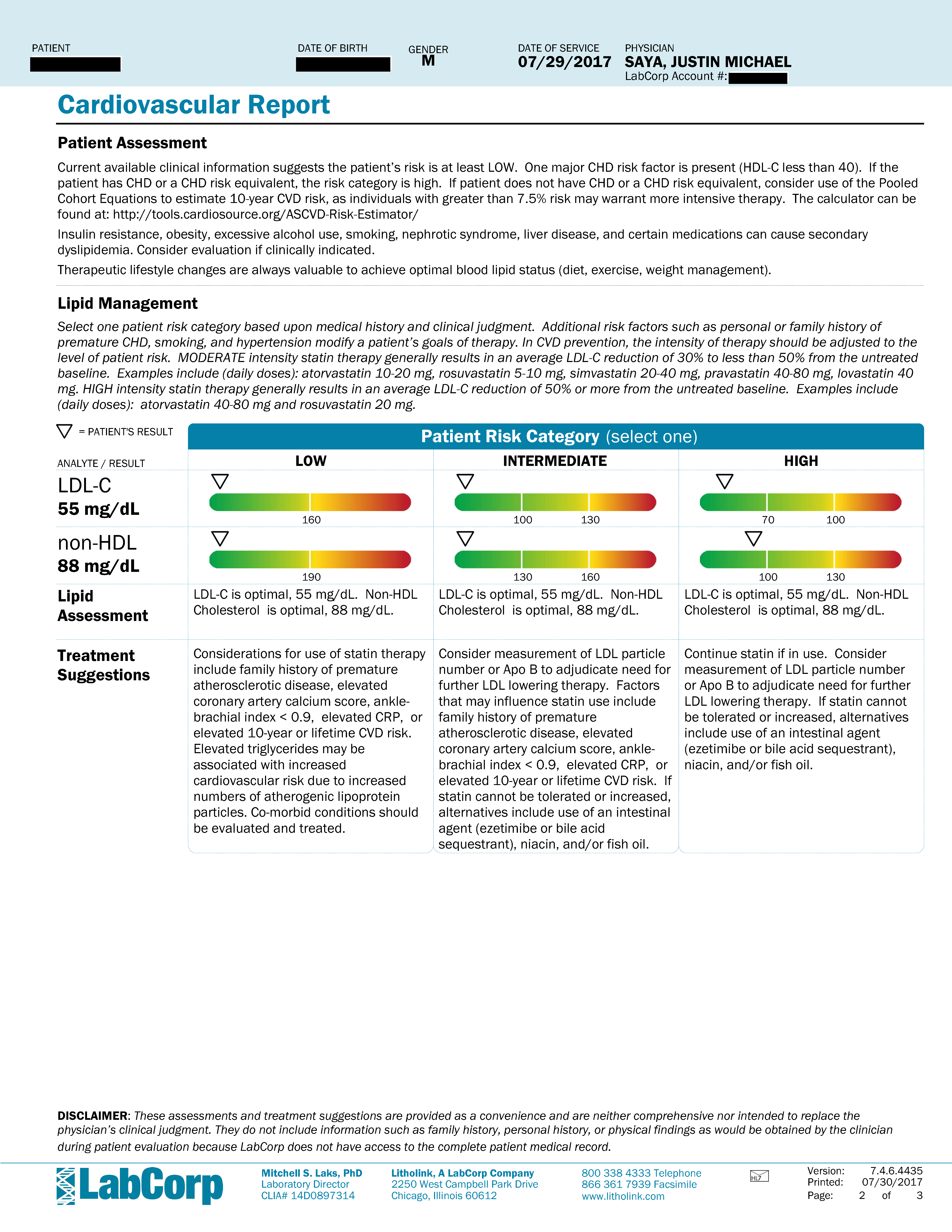
I am amazed that you can be that much overweight but have a decent lipids profile. Unless I am missing something your cardiovascular risk is low. However, your consistently elevated Glucose suggests that you could be insulin-resistant and since you are overweight that points to metabolic syndrome. Were you fasting 10-12 hours before all of the blood draws?
If so you need to get HbA1C checked
Apparently your weight gain is thyroid related?
What is the latest with you? Once you get your weight under control, thyroid function restored, and rule out diabetes you will be ready for a lot more improvement via TRT.
Hello Everyone, have been away for sometime.
Posting now with updated bloodwork and a question about Dissolving Anastrozole in vodka.
Current dosage is as follows:
.25 ml Test Cyp 3x per week
.35 ml HCG 3x per week
.25mg or 1/4 tablet 3x per week.
I have not been taking Anastrozole for several months and my blood work shows it.
Anastrozole:
I added 5 1mg tablets to 5ml of Vodka.
with (MY) dropper 34 drops = 1ml
I know the number of drops vary depending on which type of dropper you are using, Glass, plastic , ect…
I increased Vodka to 10 ml making dosage = 68 drops
68 drops x .75 = 51 drops
If 68 drops per ml, 51 drops per 3/4 or .75 ml,
17 drops 3x per week would be .75 mg / week (51=17*3)
@KSman
Is my math correct on Anastrozole dosage?
Also have apt tomorrow morning, going to ask Dr to increase Test cyp dosage.
How are you feeling? T is still low and you should probably be trying to get vit D cranked up to optimum…its pretty cheap.
You E2 isnt off the charts but you would expect it would be lower given your low T dose. Can I assume you are carrying some extra fat? I saw that you were starting to drop last year but didnt see a body weight update.
Overall am feeling well.
Vit D, was self inflicted. The last bottle of Vit D3 I purchased was only 1000IU instead of 10,000. So I will blame that on poor eyesight ![]() I have only been taking 1000iu per day. I will increase to either 5k or 10k then adjust on my next blood work.
I have only been taking 1000iu per day. I will increase to either 5k or 10k then adjust on my next blood work.
Weight has stayed the same, I was averaging 1700-1800 calories per day, Not gaining but not losing either.
On 7/15/18, I dropped to 1200 calories per day, No added sugar,only natural sugars from fruits or veggies, no Bread, no Pasta, since the 15th I have dropped 1 pound per day.
Are you being treated thyroid at all? I don’t see any ft3 or ft4 readings and your TSH is pretty high. You should be losing at those caloric levels, in fact I think they are on the low side for someone your size. 1200 is way too low to where I believe you could be doing metabolic damage. That is around the caloric level my almost 125lb wife would be at to lose weight.
I have Hypo thyroid. Doctor’s office (forgot) to add , FT3, FT4, and Reverse T3 to my script.They sent me and additional script, will do blood work in morning for the thyroid.
Also, Dr suggested if Reverse T3 numbers come back higher than 18, they would suggest starting me on Cytomel. Slowly increasing from 5mcg to 15mcg over a period of three weeks.